

Massive blood transfusion during hospitalization for delivery in New York State, 1998-2007
- PMID: 24201690
- PMCID: PMC4547558
- DOI: 10.1097/AOG.0000000000000021
Massive blood transfusion during hospitalization for delivery in New York State, 1998-2007
Abstract
Objective: To define the frequency, risk factors, and outcomes of massive transfusion in obstetrics.
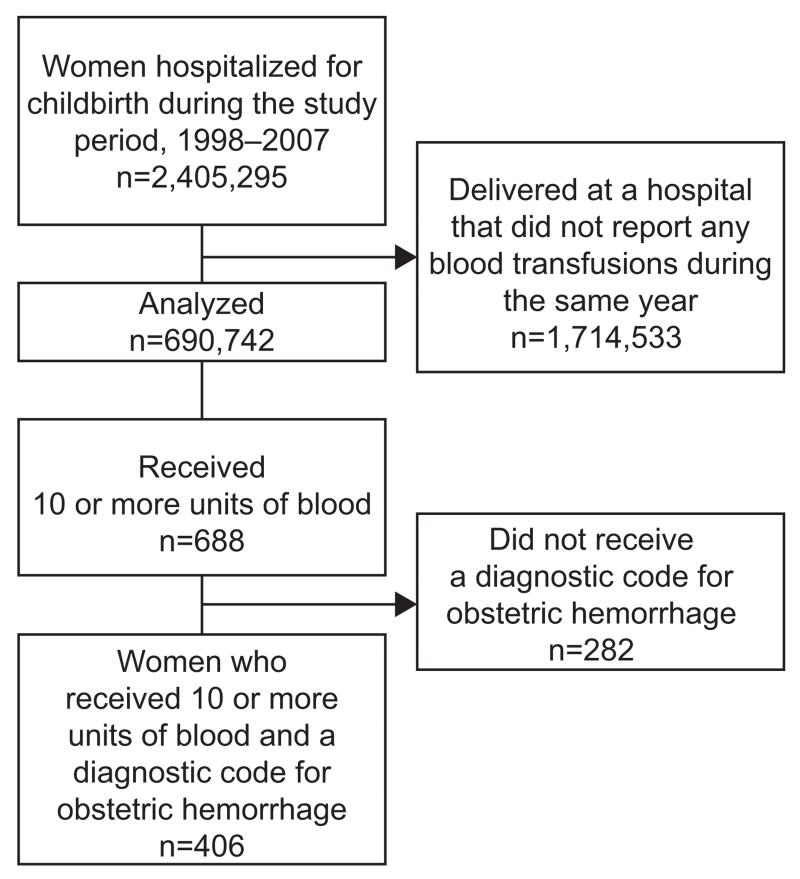
Methods: The State Inpatient Dataset for New York (1998-2007) was used to identify all delivery hospitalizations for hospitals that reported at least one delivery-related transfusion per year. Multivariable logistic regression analysis was performed to examine the relationship between maternal age, race, and relevant clinical variables and the risk of massive blood transfusion defined as 10 or more units of blood recorded.
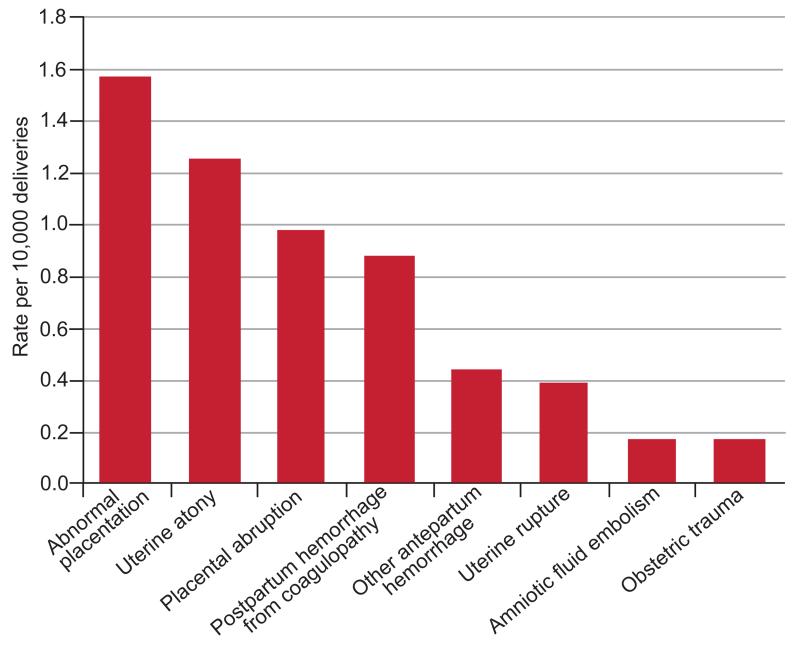
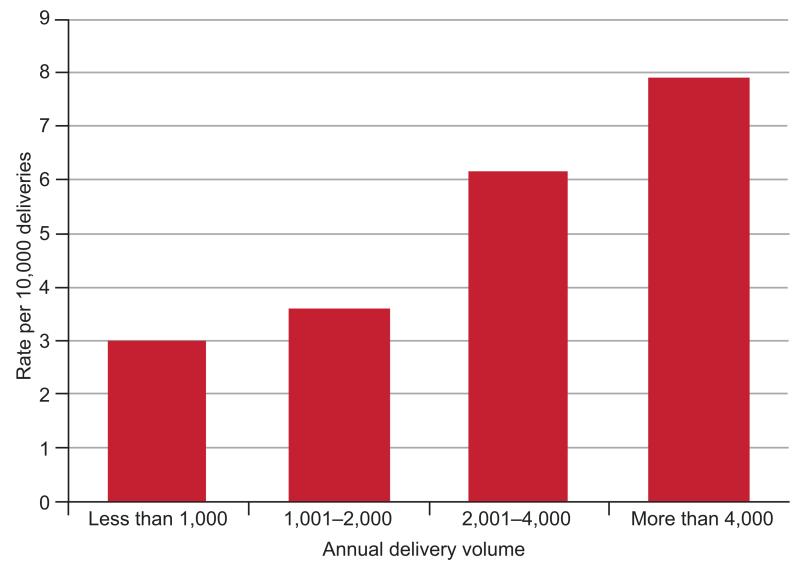
Results: Massive blood transfusion complicated 6 of every 10,000 deliveries with cases observed even in the smallest facilities. Risk factors with the strongest independent associations with massive blood transfusion included abnormal placentation (1.6/10,000 deliveries, adjusted odds ratio [OR] 18.5, 95% confidence interval [CI] 14.7-23.3), placental abruption (1.0/10,000, adjusted OR 14.6, 95% CI 11.2-19.0), severe preeclampsia (0.8/10,000, adjusted OR 10.4, 95% CI 7.7-14.2), and intrauterine fetal demise (0.7/10,000, adjusted OR 5.5, 95% CI 3.9-7.8). The most common etiologies of massive blood transfusion were abnormal placentation (26.6% of cases), uterine atony (21.2%), placental abruption (16.7%), and postpartum hemorrhage associated with coagulopathy (15.0%). A disproportionate number of women who received a massive blood transfusion experienced severe morbidity including renal failure, acute respiratory distress syndrome, sepsis, and in-hospital death.
Conclusion: Massive blood transfusion was infrequent, regardless of facility size. In the presence of known risk for receipt of massive blood transfusion, women should be informed of this possibility, should deliver in a well-resourced facility if possible, and should receive appropriate blood product preparation and venous access in advance of delivery.
Level of evidence: : II.
Figures
References
-
- Sharpe JP, Weinberg JA, Magnotti LJ, Croce MA, Fabian TC. Toward a better definition of massive transfusion: focus on the interval of hemorrhage control. J Trauma Acute Care Surg. 2012;73:1553–7. - PubMed
-
- Mitra B, Cameron PA, Gruen RL, Mori A, Fitzgerald M, Street A. The definition of massive transfusion in trauma: a critical variable in examining evidence for resuscitation. Eur J Emerg Med. 2011;18:137–42. - PubMed
-
- Skupski DW, Lowenwirt IP, Weinbaum FI, Brodsky D, Danek M, Eglinton GS. Improving hospital systems for the care of women with major obstetric hemorrhage. Obstet Gynecol. 2006;107:977–83. - PubMed
-
- Shields LE, Smalarz K, Reffigee L, Mugg S, Burdumy TJ, Propst M. Comprehensive maternal hemorrhage protocols improve patient safety and reduce utilization of blood products. Am J Obstet Gynecol. 2011;205:368, e1–8. - PubMed
-
- Eller AG, Bennett MA, Sharshiner M, Masheter C, Soisson AP, Dodson M, et al. Maternal morbidity in cases of placenta accreta managed by a multidisciplinary care team compared with standard obstetric care. Obstet Gynecol. 2011;117:331–7. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
