

The global epidemiology and contribution of cannabis use and dependence to the global burden of disease: results from the GBD 2010 study
- PMID: 24204649
- PMCID: PMC3811989
- DOI: 10.1371/journal.pone.0076635
The global epidemiology and contribution of cannabis use and dependence to the global burden of disease: results from the GBD 2010 study
Erratum in
-
Correction: The Global Epidemiology and Contribution of Cannabis Use and Dependence to the Global Burden of Disease: Results from the GBD 2010 Study.PLoS One. 2016 Oct 19;11(10):e0165221. doi: 10.1371/journal.pone.0165221. eCollection 2016. PLoS One. 2016. PMID: 27760226 Free PMC article.
Abstract
Aims: Estimate the prevalence of cannabis dependence and its contribution to the global burden of disease.
Methods: Systematic reviews of epidemiological data on cannabis dependence (1990-2008) were conducted in line with PRISMA and meta-analysis of Observational Studies in Epidemiology (MOOSE) guidelines. Culling and data extraction followed protocols, with cross-checking and consistency checks. DisMod-MR, the latest version of generic disease modelling system, redesigned as a Bayesian meta-regression tool, imputed prevalence by age, year and sex for 187 countries and 21 regions. The disability weight associated with cannabis dependence was estimated through population surveys and multiplied by prevalence data to calculate the years of life lived with disability (YLDs) and disability-adjusted life years (DALYs). YLDs and DALYs attributed to regular cannabis use as a risk factor for schizophrenia were also estimated.
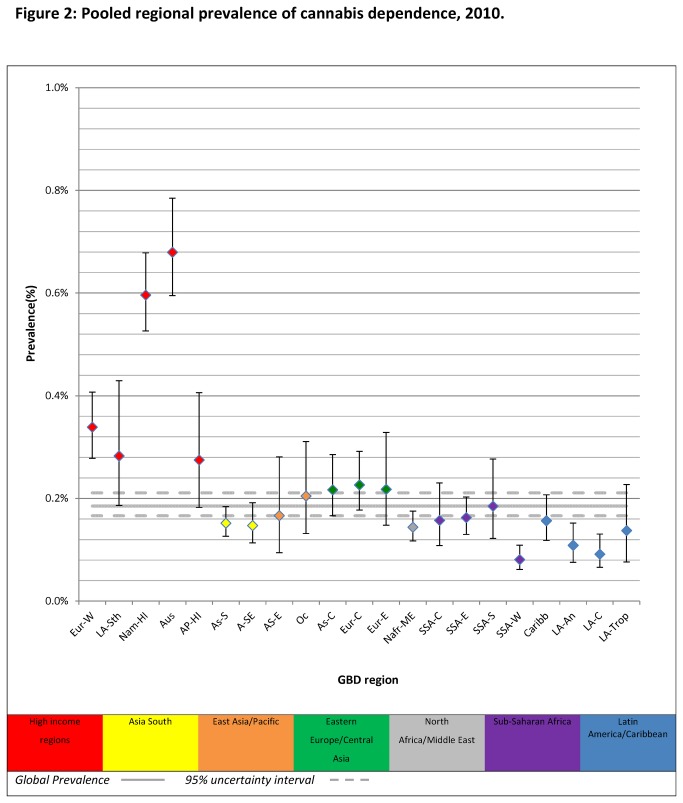
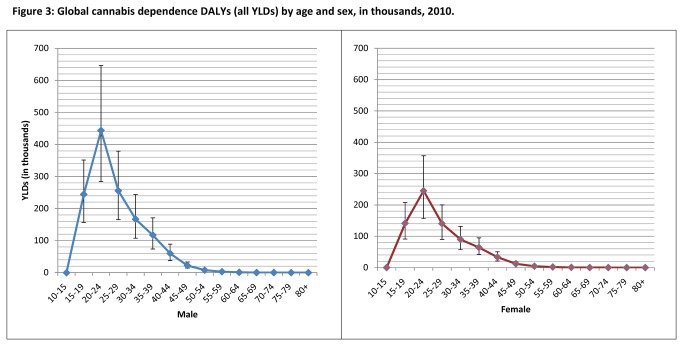
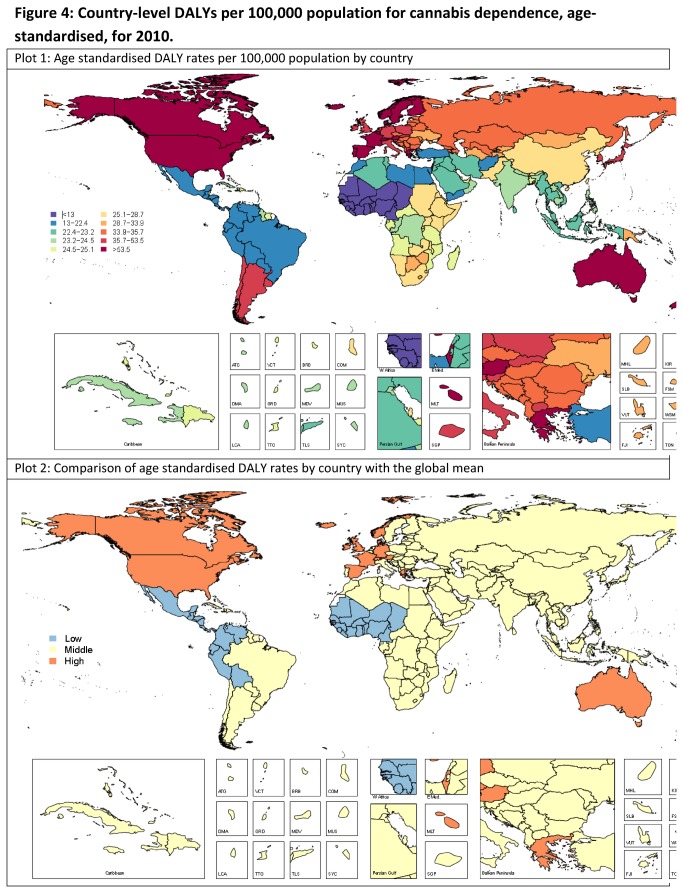
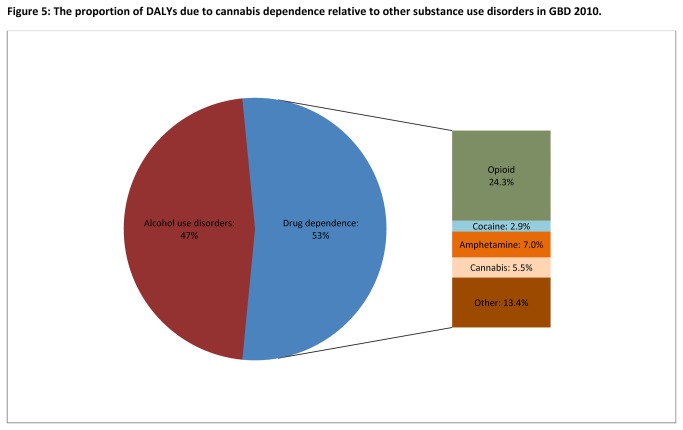
Results: There were an estimated 13.1 million cannabis dependent people globally in 2010 (point prevalence0.19% (95% uncertainty: 0.17-0.21%)). Prevalence peaked between 20-24 yrs, was higher in males (0.23% (0.2-0.27%)) than females (0.14% (0.12-0.16%)) and in high income regions. Cannabis dependence accounted for 2 million DALYs globally (0.08%; 0.05-0.12%) in 2010; a 22% increase in crude DALYs since 1990 largely due to population growth. Countries with statistically higher age-standardised DALY rates included the United States, Canada, Australia, New Zealand and Western European countries such as the United Kingdom; those with lower DALY rates were from Sub-Saharan Africa-West and Latin America. Regular cannabis use as a risk factor for schizophrenia accounted for an estimated 7,000 DALYs globally.
Conclusion: Cannabis dependence is a disorder primarily experienced by young adults, especially in higher income countries. It has not been shown to increase mortality as opioid and other forms of illicit drug dependence do. Our estimates suggest that cannabis use as a risk factor for schizophrenia is not a major contributor to population-level disease burden.
Conflict of interest statement
Figures

References
-
- Gaoni Y, Mechoulam R (1964) Isolation, structure, and partial synthesis of an active constituent of hashish. J Am Chem Soc 86: 1646-1647. doi:10.1021/ja01062a046. - DOI
-
- Martin B, Cone E (1999) Chemistry and pharmacology of cannabis. In: Kalant H, Corrigal W, Hall W, Smart R. The Health Effects of Cannabis. Toronto: Addiction Research Foundation; pp. 19-68.
-
- Iversen LL (2000) The science of marijuana. Oxford University Press.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
