

New oral anticoagulants are not superior to warfarin in secondary prevention of stroke or transient ischemic attacks, but lower the risk of intracranial bleeding: insights from a meta-analysis and indirect treatment comparisons
- PMID: 24204920
- PMCID: PMC3808395
- DOI: 10.1371/journal.pone.0077694
New oral anticoagulants are not superior to warfarin in secondary prevention of stroke or transient ischemic attacks, but lower the risk of intracranial bleeding: insights from a meta-analysis and indirect treatment comparisons
Abstract
Purpose: Patients with Atrial Fibrillation (AF) and prior stroke are classified as high risk in all risk stratification schemes. A systematic review and meta-analysis was performed to compare the efficacy and safety of New Oral Anticoagulants (NOACs) to warfarin in patients with AF and previous stroke or transient ischemic attack (TIA).
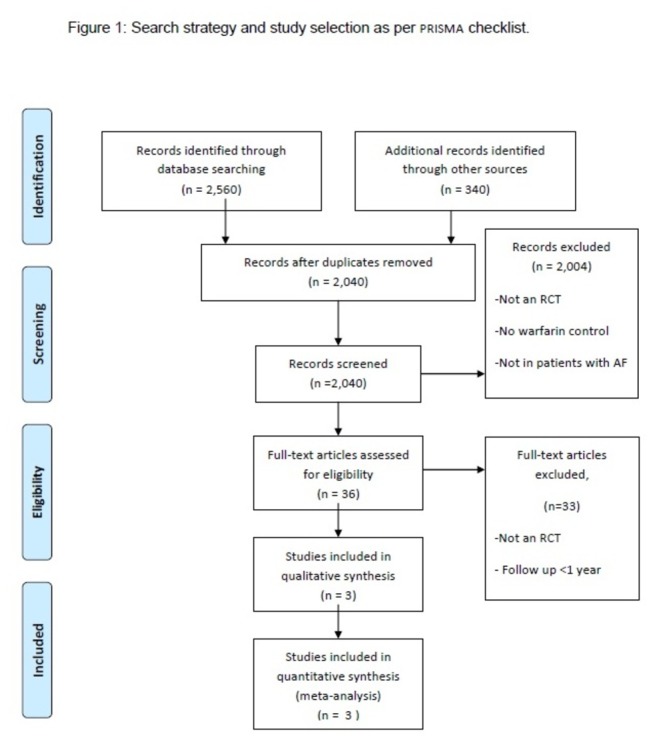
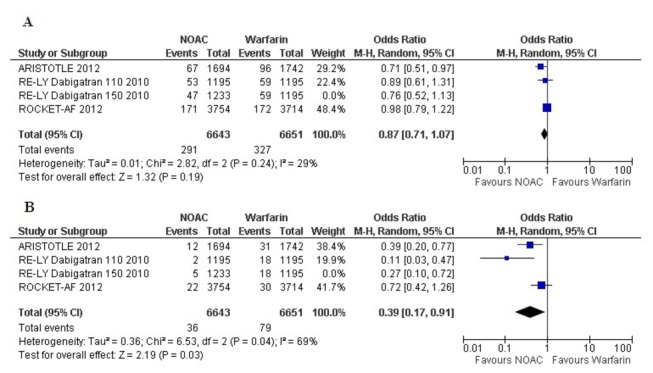
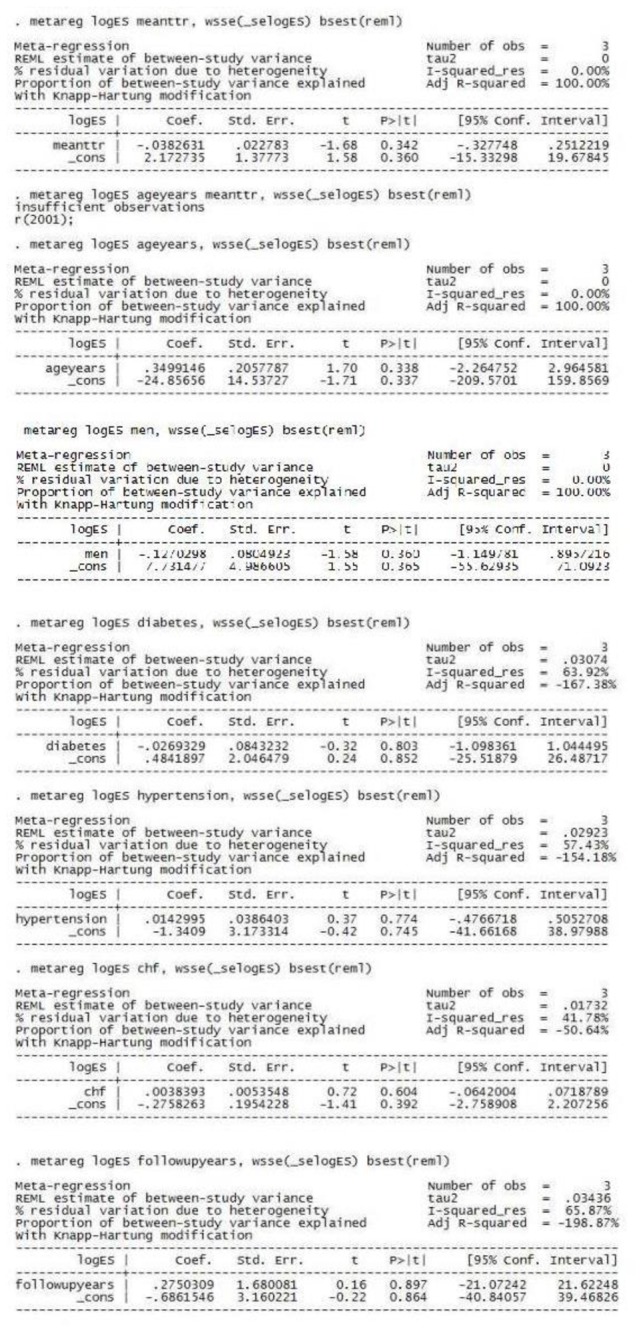
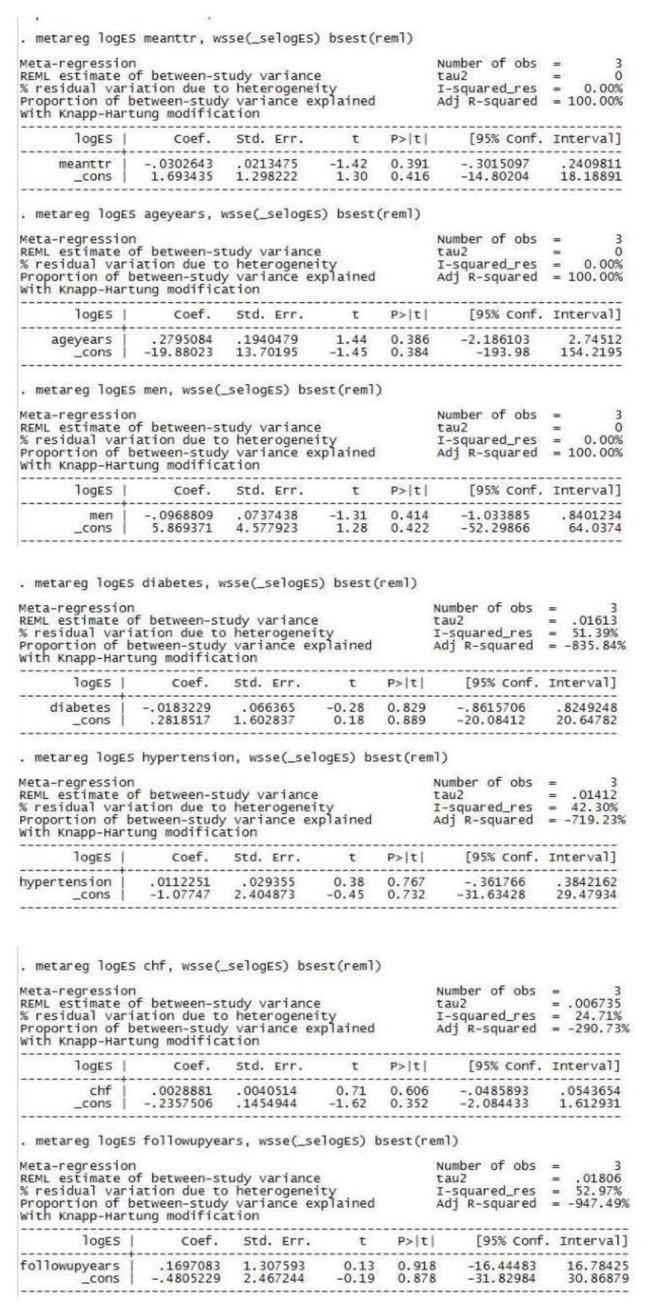
Methods: Three randomized controlled trials (RCTs), including total 14527 patients, comparing NOACs (apixaban, dabigatran and rivaroxaban) with warfarin were included in the analysis. Primary efficacy endpoint was ischemic stroke, and primary safety endpoint was intracranial bleeding. Random-effects models were used to pool efficacy and safety data across RCTs. RevMan and Stata software were used for direct and indirect comparisons, respectively.
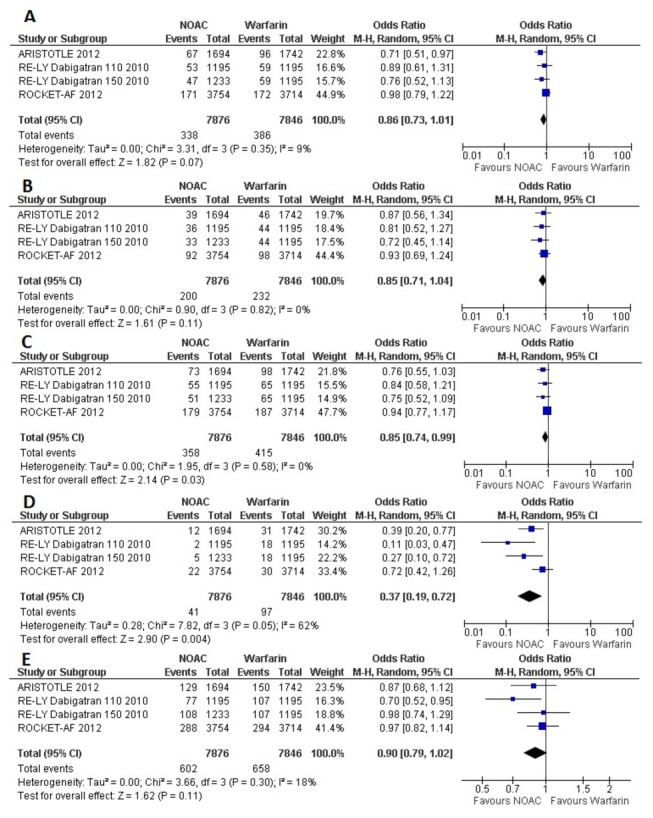
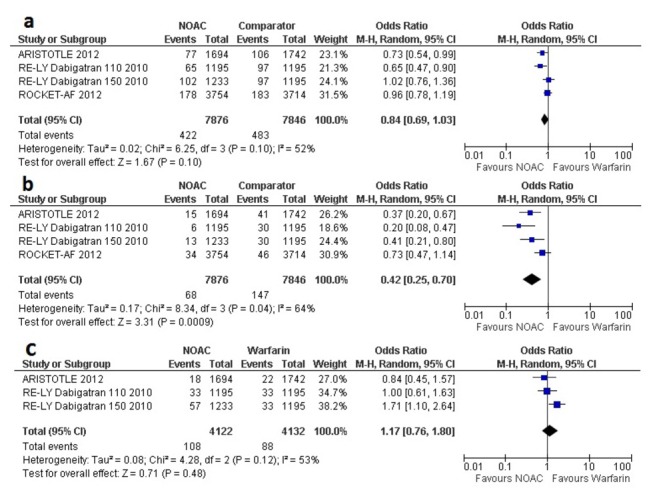
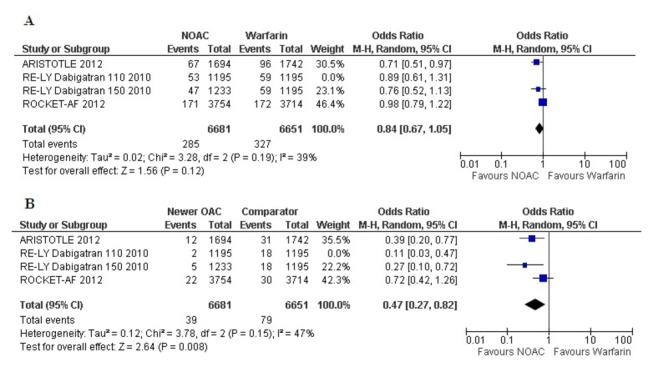
Results: In patients with AF and previous stroke or TIA, effects of NOACs were not statistically different from that of warfarin, in reduction of stroke (Odds Ratio [OR] 0.86, 95% confidence interval [CI] 0.73- 1.01), disabling and fatal stroke (OR 0.85, 95% CI 0.71-1.04), and all-cause mortality (OR 0.90, 95% CI 0.79 -1.02). Randomization to NOACs was associated with a significantly lower risk of intracranial bleeding (OR 0.42, 95% CI 0.25-0.70). There were no major differences in efficacy between apixaban, dabigatran (110 mg BID and 150 mg BID) and rivaroxaban. Major bleeding was significantly lower with apixaban and dabigatran (110 mg BID) compared with dabigatran (150 mg BID) and rivaroxaban.
Conclusion: NOACs may not be more effective than warfarin in the secondary prevention of ischemic stroke in patients with a prior history of cerebrovascular ischemia, but have a lower risk of intracranial bleeding.
Conflict of interest statement
Figures
Similar articles
-
Nonvitamin-K-antagonist oral anticoagulants versus warfarin in patients with atrial fibrillation and previous stroke or transient ischemic attack: An updated systematic review and meta-analysis of randomized controlled trials.Int J Stroke. 2017 Aug;12(6):589-596. doi: 10.1177/1747493017700663. Epub 2017 Mar 15. Int J Stroke. 2017. PMID: 28730948
-
Indirect comparisons of new oral anticoagulant drugs for efficacy and safety when used for stroke prevention in atrial fibrillation.J Am Coll Cardiol. 2012 Aug 21;60(8):738-46. doi: 10.1016/j.jacc.2012.03.019. Epub 2012 May 9. J Am Coll Cardiol. 2012. PMID: 22575324
-
Efficacy and safety of edoxaban in comparison with dabigatran, rivaroxaban and apixaban for stroke prevention in atrial fibrillation. An indirect comparison analysis.Thromb Haemost. 2014 May 5;111(5):981-8. doi: 10.1160/TH14-02-0118. Epub 2014 Feb 28. Thromb Haemost. 2014. PMID: 24577485
-
Effectiveness and Safety of Apixaban, Dabigatran, and Rivaroxaban Versus Warfarin in Patients With Nonvalvular Atrial Fibrillation and Previous Stroke or Transient Ischemic Attack.Stroke. 2017 Aug;48(8):2142-2149. doi: 10.1161/STROKEAHA.117.017474. Epub 2017 Jun 27. Stroke. 2017. PMID: 28655814
-
Non-vitamin-K oral anticoagulants (NOACs) for the prevention of secondary stroke.Expert Opin Pharmacother. 2018 Oct;19(14):1597-1602. doi: 10.1080/14656566.2018.1515913. Epub 2018 Sep 17. Expert Opin Pharmacother. 2018. PMID: 30152249 Review.
Cited by
-
Early introduction of direct oral anticoagulants in cardioembolic stroke patients with non-valvular atrial fibrillation.J Thromb Thrombolysis. 2016 Oct;42(3):393-8. doi: 10.1007/s11239-016-1393-9. J Thromb Thrombolysis. 2016. PMID: 27329483
-
Secondary Prevention with Antithrombotic Therapies in Stable Ischemic Heart Disease Patients: a Review.Curr Cardiol Rep. 2019 May 18;21(7):56. doi: 10.1007/s11886-019-1152-6. Curr Cardiol Rep. 2019. PMID: 31104152 Review.
-
The Role of Nonvitamin K Antagonist Oral Anticoagulants (NOACs) in Stroke Prevention in Patients with Atrial Fibrillation.Curr Neurol Neurosci Rep. 2016 May;16(5):47. doi: 10.1007/s11910-016-0645-6. Curr Neurol Neurosci Rep. 2016. PMID: 27023335 Review.
-
Efficacy and Safety of Direct Oral Anticoagulants (DOACs) Versus Warfarin in Atrial Fibrillation Patients with Prior Stroke: a Systematic Review and Meta-analysis.Cardiovasc Drugs Ther. 2023 Dec;37(6):1225-1237. doi: 10.1007/s10557-022-07336-w. Epub 2022 Apr 25. Cardiovasc Drugs Ther. 2023. PMID: 35467313
-
Direct oral anticoagulants in the secondary prevention of stroke and transient ischemic attack in patients with atrial fibrillation.Intern Emerg Med. 2015 Aug;10(5):555-60. doi: 10.1007/s11739-015-1226-4. Epub 2015 Apr 11. Intern Emerg Med. 2015. PMID: 25862436 Review.
References
-
- Fang MC, Go AS, Chang Y, Borowsky L, Pomernacki NK et al. (2008) ATRIA Study Group. Comparison of risk stratification schemes to predict thromboembolism in people with nonvalvular atrial fibrillation. J Am Coll Cardiol 51: 810-815. doi:10.1016/j.jacc.2007.09.065. PubMed: 18294564. - DOI - PMC - PubMed
-
- Saxena R, Koudstaal P (2004) Anticoagulants versus antiplatelet therapy for preventing stroke in patients with nonrheumatic atrial fibrillation and a history of stroke or transient ischemic attack. Cochrane Database Syst Rev 4: CD000187. - PubMed
-
- De Caterina R, Husted S, Wallentin L, Andreotti F, Arnesen H et al. (2012) Coordinating Committee. New oral anticoagulants in atrial fibrillation and acute coronary syndromes: ESC Working Group on Thrombosis-Task Force on Anticoagulants in Heart Disease position paper. J Am Coll Cardiol 59: 1413-1425. doi:10.1016/S0735-1097(12)61414-4. PubMed: 22497820. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
