

Efficacy and safety of intravitreal therapy in macular edema due to branch and central retinal vein occlusion: a systematic review
- PMID: 24205253
- PMCID: PMC3808377
- DOI: 10.1371/journal.pone.0078538
Efficacy and safety of intravitreal therapy in macular edema due to branch and central retinal vein occlusion: a systematic review
Abstract
Background: Intravitreal agents have replaced observation in macular edema in central (CRVO) and grid laser photocoagulation in branch retinal vein occlusion (BRVO). We conducted a systematic review to evaluate efficacy and safety outcomes of intravitreal therapies for macular edema in CRVO and BRVO.
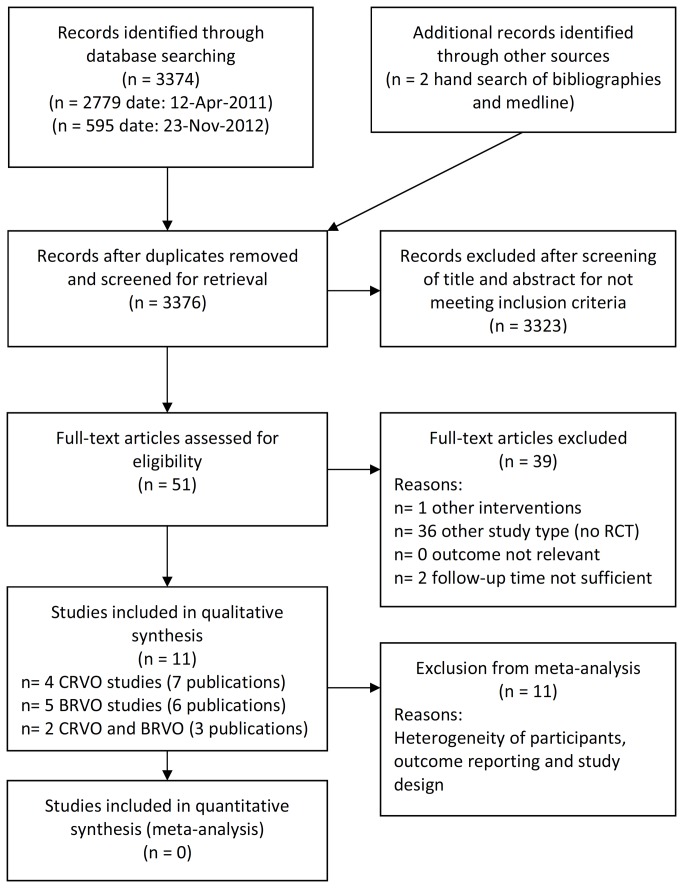
Methods and findings: MEDLINE, Embase, and the Cochrane Library were systematically searched for RCTs with no limitations of language and year of publication. 11 RCTs investigating anti-VEGF agents (ranibizumab, bevacizumab, aflibercept) and steroids (triamcinolone, dexamethasone implant) with a minimum follow-up of 1 year were evaluated.
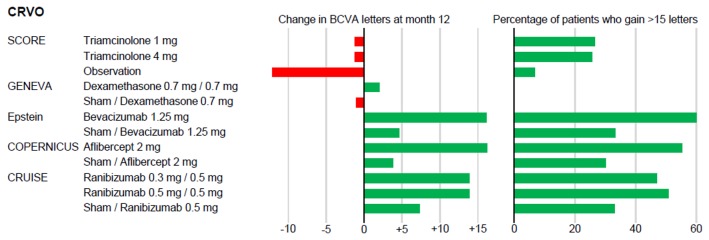
Efficacy crvo: Greatest gain in visual acuity after 12 months was observed both under aflibercept 2 mg: +16.2 letters (8.5 injections), and under bevacizumab 1.25 mg: +16.1 letters (8 injections). Ranibizumab 0.5 mg improved vision by +13.9 letters (8.8 injections). Triamcinolone 1 mg and 4 mg stabilized visual acuity at a lower injection frequency (-1.2 letters, 2 injections).
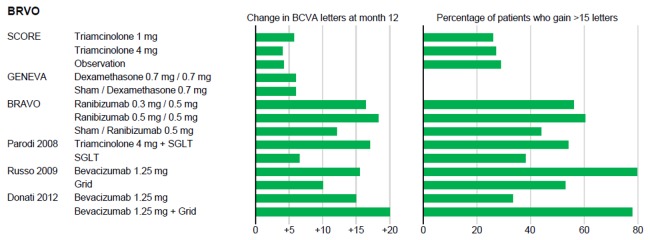
Brvo: Ranibizumab 0.5 mg resulted in a visual acuity gain of +18.3 letters (8.4 injections). The effect of dexamethasone implant was transient after 1.9 implants in both indications.
Safety: Serious ocular adverse events were rare, e.g., endophthalmitis occurred in 0.0-0.9%. Major differences were found in an indirect comparison between steroids and anti-VEGF agents for cataract progression (19.8-35.0% vs. 0.9-7.0%) and in required treatment of increased intraocular pressure (7.0-41.0% vs. none). No major differences were identified in systemic adverse events.
Conclusions: Anti-VEGF agents result in a promising gain of visual acuity, but require a high injection frequency. Dexamethasone implant might be an alternative, but comparison is impaired as the effect is temporary and it has not yet been tested in PRN regimen. The ocular risk profile seems to be favorable for anti-VEGF agents in comparison to steroids. Because comparative data from head-to-head trials are missing currently, clinicians and patients should carefully weigh the benefit-harm ratio.
Conflict of interest statement
Figures
References
-
- Scott IU, Ip MS, VanVeldhuisen PC, Oden NL, Blodi BA et al. ; (2009) A randomized trial comparing the efficacy and safety of intravitreal triamcinolone with standard care to treat vision loss associated with macular Edema secondary to branch retinal vein occlusion: the Standard Care vs Corticosteroid for Retinal Vein Occlusion (SCORE) Study report 6 Arch Ophthalmol 127: 1115–1128 doi:10.1001/archophthalmol.2009.233. - PMC - PubMed
-
- Ip MS, Scott IU, VanVeldhuisen PC, Oden NL, Blodi BA et al. ; (2009) A randomized trial comparing the efficacy and safety of intravitreal triamcinolone with observation to treat vision loss associated with macular edema secondary to central retinal vein occlusion: the Standard Care vs Corticosteroid for Retinal Vein Occlusion (SCORE) Study report 5 Arch Ophthalmol 127: 1101–1114 doi:10.1001/archophthalmol.2009.234. - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
