Reduction glossectomy for large tongues
- PMID: 24205477
- PMCID: PMC3814666
- DOI: 10.4103/2231-0746.119230
Reduction glossectomy for large tongues
Abstract
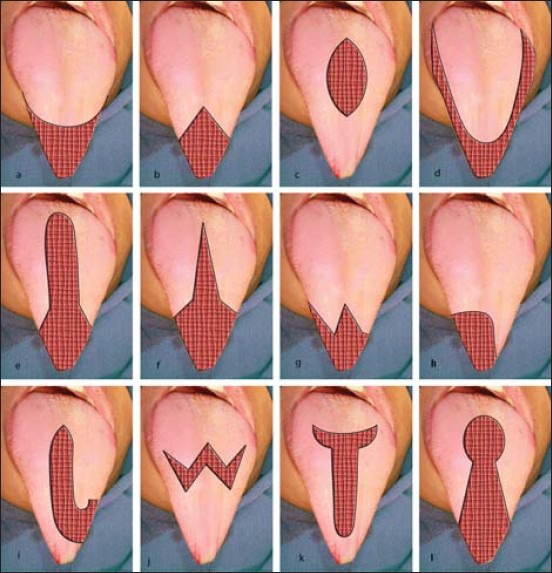
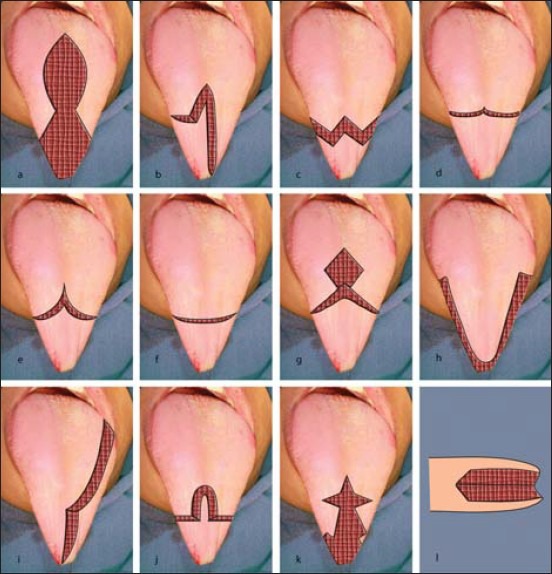
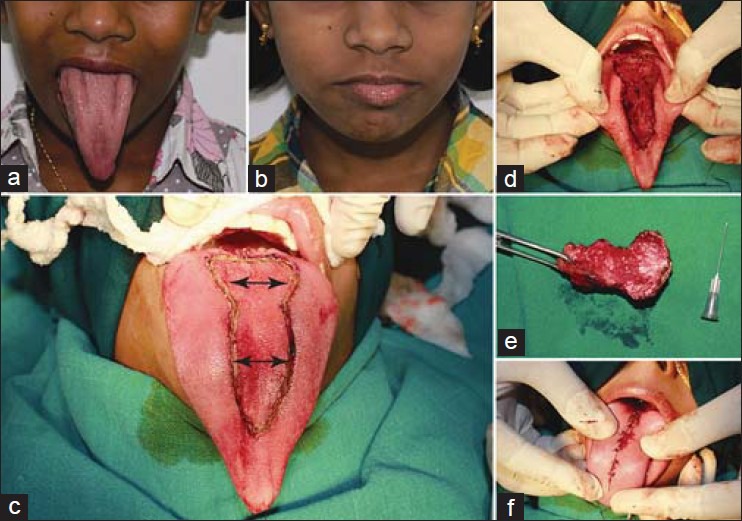
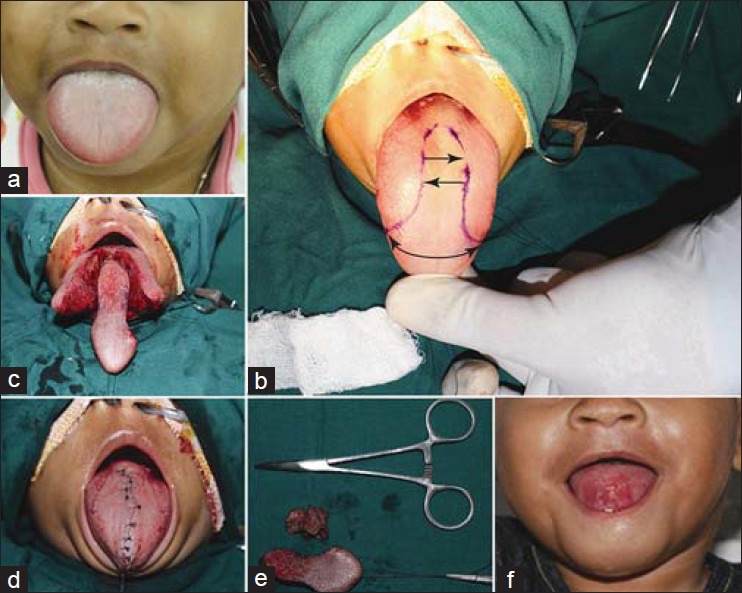
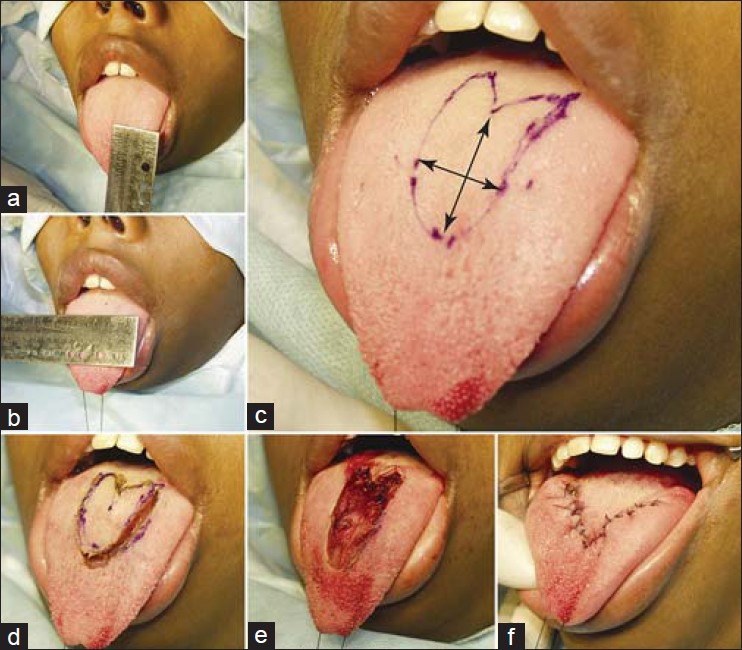
Pathological enlargement of tongue is caused by several conditions and diseases. In several instances, surgery remains the only viable option for complete cure. Persistent bleeding, compromised neuro-motor-sensory functions during the postoperative period are the most common complaints encountered after macroglossia correction. The tongue is a muscular organ, whose complex neuroanatomy is being unraveled slowly. Various types of macroglossia resections in unique clinical situations have been proposed by several clinicians till date. There has never been unanimously accepted resection for the treatment of macroglossia. This review article attempts to preview the cosmetic and functional components for resection designs.
Keywords: Beckwith-Wiedemann syndrome; macroglossia; neuroanatomy; tongue musculature; tongue resection.
Conflict of interest statement
Figures
References
-
- Prada CE, Zarate YA, Hopkin RJ. Genetic Causes of Macroglossia: Diagnostic Approach. Pediatrics. 2012;129:e431–37. - PubMed
-
- Weiss LS, White JA. Macroglossia: A review. J La State Med Soc. 1990;142:13–6. - PubMed
-
- Ueyama Y, Mano T, Nishiyama A, Tsukamoto G, Shintani S, Matsumura T. Effects of surgical reduction of the tongue. Br J OralMaxillofac Surg. 1999;37:490–5. - PubMed
-
- Ruscello DM, Douglas C, Tyson T, Durkee M. Macroglossia: A case study. J Commun Disord. 2005;38:109–22. - PubMed
-
- Myer CM, 3rd, Hotaling AJ, Reilly JS. The diagnosis and treatment of macroglossia in children. Ear Nose Throat J. 1986;65:444–8. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources