

APOL1 risk variants, race, and progression of chronic kidney disease
- PMID: 24206458
- PMCID: PMC3969022
- DOI: 10.1056/NEJMoa1310345
APOL1 risk variants, race, and progression of chronic kidney disease
Abstract
Background: Among patients in the United States with chronic kidney disease, black patients are at increased risk for end-stage renal disease, as compared with white patients.
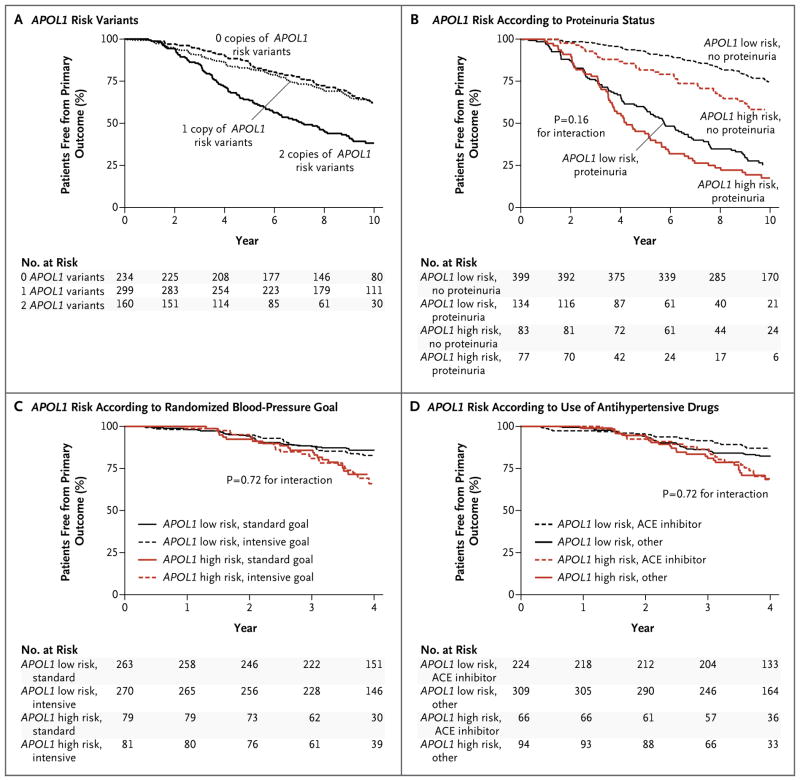
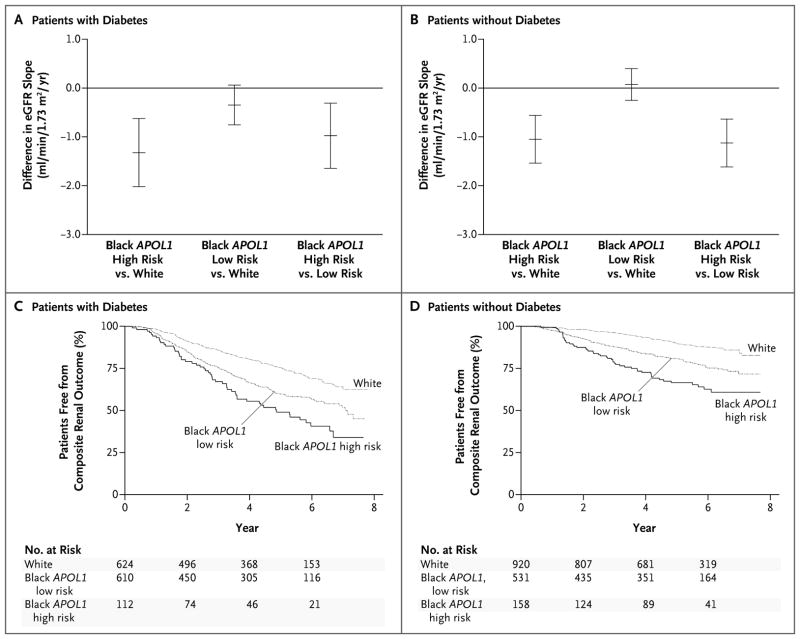
Methods: In two studies, we examined the effects of variants in the gene encoding apolipoprotein L1 (APOL1) on the progression of chronic kidney disease. In the African American Study of Kidney Disease and Hypertension (AASK), we evaluated 693 black patients with chronic kidney disease attributed to hypertension. In the Chronic Renal Insufficiency Cohort (CRIC) study, we evaluated 2955 white patients and black patients with chronic kidney disease (46% of whom had diabetes) according to whether they had 2 copies of high-risk APOL1 variants (APOL1 high-risk group) or 0 or 1 copy (APOL1 low-risk group). In the AASK study, the primary outcome was a composite of end-stage renal disease or a doubling of the serum creatinine level. In the CRIC study, the primary outcomes were the slope in the estimated glomerular filtration rate (eGFR) and the composite of end-stage renal disease or a reduction of 50% in the eGFR from baseline.
Results: In the AASK study, the primary outcome occurred in 58.1% of the patients in the APOL1 high-risk group and in 36.6% of those in the APOL1 low-risk group (hazard ratio in the high-risk group, 1.88; P<0.001). There was no interaction between APOL1 status and trial interventions or the presence of baseline proteinuria. In the CRIC study, black patients in the APOL1 high-risk group had a more rapid decline in the eGFR and a higher risk of the composite renal outcome than did white patients, among those with diabetes and those without diabetes (P<0.001 for all comparisons).
Conclusions: Renal risk variants in APOL1 were associated with the higher rates of end-stage renal disease and progression of chronic kidney disease that were observed in black patients as compared with white patients, regardless of diabetes status. (Funded by the National Institute of Diabetes and Digestive and Kidney Diseases and others.).
Figures
Comment in
-
Health disparities in kidney disease--emerging data from the human genome.N Engl J Med. 2013 Dec 5;369(23):2260-1. doi: 10.1056/NEJMe1312797. Epub 2013 Nov 9. N Engl J Med. 2013. PMID: 24206461 No abstract available.
References
-
- McClellan W, Tuttle E, Issa A. Racial differences in the incidence of hypertensive end-stage renal disease (ESRD) are not entirely explained by differences in the prevalence of hypertension. Am J Kidney Dis. 1988;12:285–90. - PubMed
-
- Cowie CC, Port FK, Wolfe RA, Savage PJ, Moll PP, Hawthorne VM. Disparities in incidence of diabetic end-stage renal disease according to race and type of diabetes. N Engl J Med. 1989;321:1074–9. - PubMed
-
- Hall YN, Hsu CY, Iribarren C, Darbinian J, McCulloch CE, Go AS. The conundrum of increased burden of end-stage renal disease in Asians. Kidney Int. 2005;68:2310–6. - PubMed
-
- Hsu CY, Lin F, Vittinghoff E, Shlipak MG. Racial differences in the progression from chronic renal insufficiency to end-stage renal disease in the United States. J Am Soc Nephrol. 2003;14:2902–7. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- U01 DK060963/DK/NIDDK NIH HHS/United States
- UL1 RR024131/RR/NCRR NIH HHS/United States
- U01DK061028/DK/NIDDK NIH HHS/United States
- UL1 RR029887/RR/NCRR NIH HHS/United States
- K24 DK002818/DK/NIDDK NIH HHS/United States
- M01 RR-00071/RR/NCRR NIH HHS/United States
- UL1 RR024134/RR/NCRR NIH HHS/United States
- U01 DK061028/DK/NIDDK NIH HHS/United States
- UL1 RR-025005/RR/NCRR NIH HHS/United States
- UL1 RR-024989/RR/NCRR NIH HHS/United States
- DK 2818-02/DK/NIDDK NIH HHS/United States
- UL1 RR024989/RR/NCRR NIH HHS/United States
- K12 RR023250/RR/NCRR NIH HHS/United States
- HHSN26120080001E/PHS HHS/United States
- R01 DK072231/DK/NIDDK NIH HHS/United States
- U01DK060963/DK/NIDDK NIH HHS/United States
- P20-RR11145/RR/NCRR NIH HHS/United States
- UL1 RR025005/RR/NCRR NIH HHS/United States
- M01 RR-00080/RR/NCRR NIH HHS/United States
- U01 DK060984/DK/NIDDK NIH HHS/United States
- U01 DK061021/DK/NIDDK NIH HHS/United States
- RR029887/RR/NCRR NIH HHS/United States
- UL1 RR-029879/RR/NCRR NIH HHS/United States
- U01DK061022/DK/NIDDK NIH HHS/United States
- P20 RR011104/RR/NCRR NIH HHS/United States
- UL1 RR-024131/RR/NCRR NIH HHS/United States
- P30 GM103337/GM/NIGMS NIH HHS/United States
- U01 DK060980/DK/NIDDK NIH HHS/United States
- M01 RR00827/RR/NCRR NIH HHS/United States
- M01 RR000071/RR/NCRR NIH HHS/United States
- P20 RR011145/RR/NCRR NIH HHS/United States
- U01DK060980/DK/NIDDK NIH HHS/United States
- U01 DK061022/DK/NIDDK NIH HHS/United States
- U01DK061021/DK/NIDDK NIH HHS/United States
- U01DK060984/DK/NIDDK NIH HHS/United States
- U01DK060990/DK/NIDDK NIH HHS/United States
- UL1 TR000439/TR/NCATS NIH HHS/United States
- M01 RR000052/RR/NCRR NIH HHS/United States
- M01 RR016500/RR/NCRR NIH HHS/United States
- U01 DK060902/DK/NIDDK NIH HHS/United States
- ImNIH/Intramural NIH HHS/United States
- UL1 TR-000439/TR/NCATS NIH HHS/United States
- U01DK060902/DK/NIDDK NIH HHS/United States
- 2P20 RR11104/RR/NCRR NIH HHS/United States
- U01 DK060990/DK/NIDDK NIH HHS/United States
- UL1 RR-024134/RR/NCRR NIH HHS/United States
- M0100032/PHS HHS/United States
- M01 RR-16500/RR/NCRR NIH HHS/United States
- UL1 RR-024986/RR/NCRR NIH HHS/United States
- M01 RR000827/RR/NCRR NIH HHS/United States
- M01 RR000080/RR/NCRR NIH HHS/United States
- M01 RR00052/RR/NCRR NIH HHS/United States
- UL1 RR024986/RR/NCRR NIH HHS/United States
- UL1 RR029879/RR/NCRR NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous