

Mild expression of mitral valve prolapse in the Framingham offspring: expanding the phenotypic spectrum
- PMID: 24206636
- PMCID: PMC4239996
- DOI: 10.1016/j.echo.2013.09.015
Mild expression of mitral valve prolapse in the Framingham offspring: expanding the phenotypic spectrum
Abstract
Background: Mitral valve (MV) prolapse (MVP) is a common disorder associated with mitral regurgitation, endocarditis, heart failure, and sudden death. Nondiagnostic morphologies have been described in the familial context and may represent early expression of MVP in those genetically predisposed. The aim of this study was to explore the spectrum of MVP abnormalities in the community and compare their clinical and echocardiographic features.
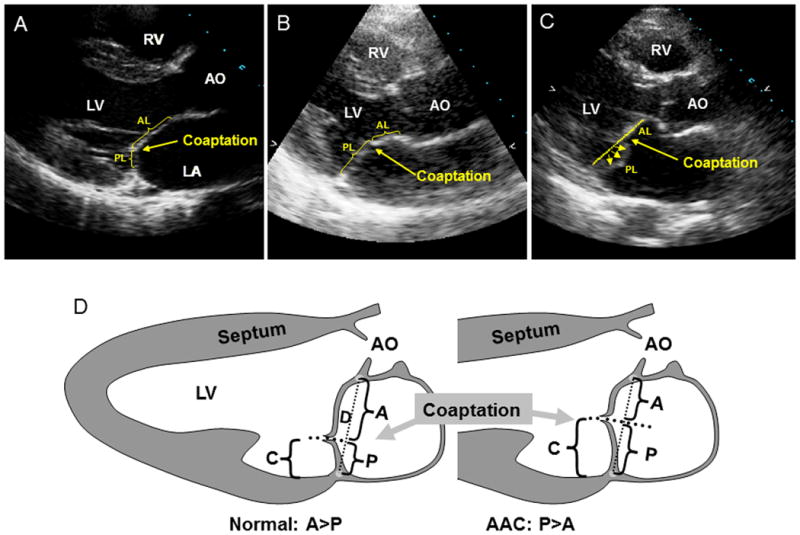
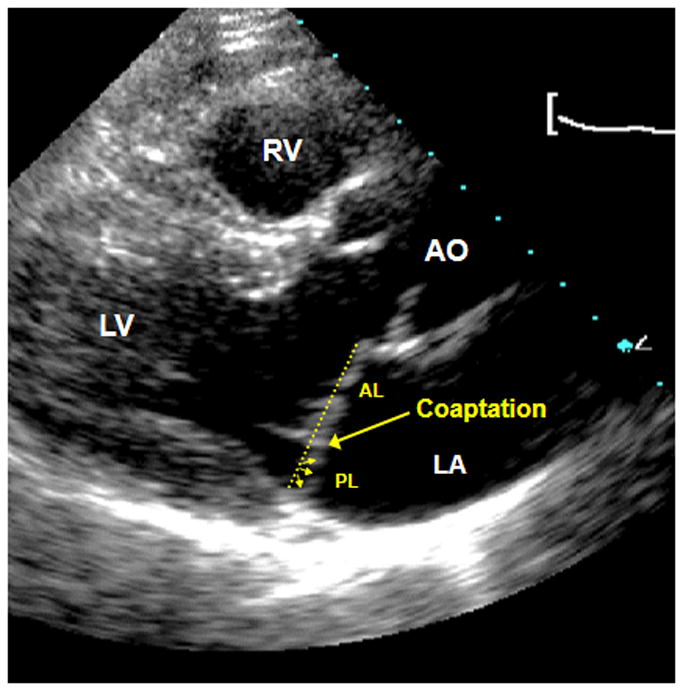
Methods: We measured annular diameter MV leaflet displacement, thickness, anterior and posterior leaflet projections onto the annulus, MV leaflet coaptation height (posterior MV leaflet projection/annular diameter), and MR jet height in 296 individuals of the Framingham Offspring Study with MVP (n = 77), the "abnormal anterior coaptation" (AAC) phenotype (n = 11) or "minimal systolic displacement" (MSD) (n = 57), and 151 age-matched and sex-matched referents with no MVP or its nondiagnostic forms.
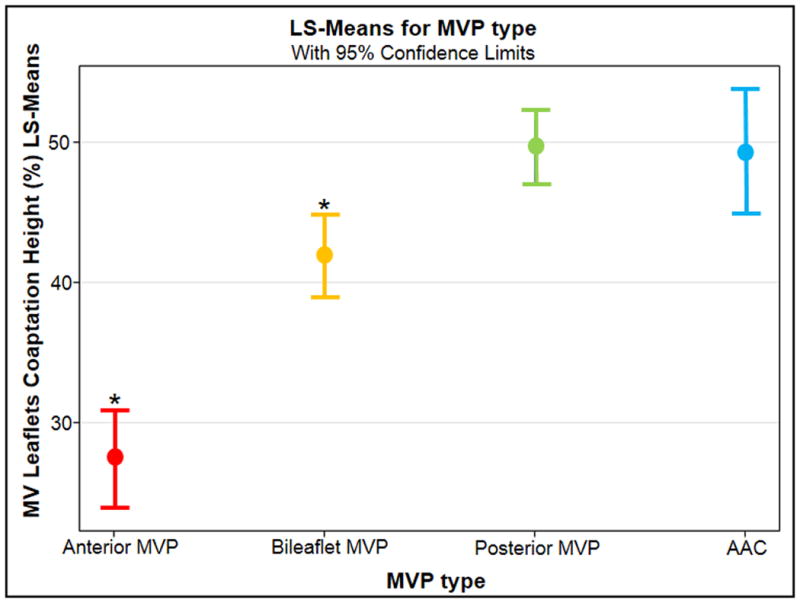
Results: AAC did not meet diagnostic displacement criteria but resembled MVP with regard to annular diameter and leaflet thickness (P > .05 for both). AAC was similar to posterior MVP with regard to posterior leaflet asymmetry and an anteriorly shifted coaptation (P = .91). Compared to patients with MSD and referents, patients with AAC had greater leaflet coaptation height, thickness, and annular diameter (P < .05 for all). MSD shared the posterior leaflet asymmetry with MVP, but the coaptation point was more posterior (coaptation height = 31% vs. 42%, P < .0001), as seen in referents. A higher proportion of patients with MVP had jet height ≥ 2 mm (mild or greater MR) compared with the other participants (44% vs. 16%, P < .0001).
Conclusions: Nondiagnostic morphologies are observed in the community and share the common feature of posterior leaflet asymmetry with MVP. AAC and MSD may thus represent early expressions of MVP. Longitudinal studies are warranted to elucidate the natural history of these phenotypes.
Keywords: AAC; Abnormal anterior coaptation; Echocardiography; FHS; Framingham Heart Study; JH; LV; Left ventricular; MR; MSD; MV; MVP; Minimal systolic displacement; Mitral regurgitation; Mitral regurgitation jet height; Mitral valve; Mitral valve prolapse.
Published by Mosby, Inc.
Figures
References
-
- Devereux RB, Jones EC, Roman MJ, Howard BV, Fabsitz RR, Liu JE, Palmieri V, Welty TK, Lee ET. Prevalence and correlates of mitral valve prolapse in a population-based sample of American Indians: the Strong Heart Study. Am J Med. 2001;111(9):679–685. - PubMed
-
- Freed LA, Benjamin EJ, Levy D, Larson MG, Evans JC, Fuller DL, Lehman B, Levine RA. Mitral valve prolapse in the general population: the benign nature of echocardiographic features in the Framingham Heart Study. J Am Coll Cardiol. 2002;40(7):1298–1304. - PubMed
-
- Freed LA, Levy D, Levine RA, Larson MG, Evans JC, Fuller DL, Lehman B, Benjamin EJ. Prevalence and clinical outcome of mitral-valve prolapse. N Engl J Med. 1999;341(1):1–7. - PubMed
-
- Rabkin E, Aikawa M, Stone JR, Fukumoto Y, Libby P, Schoen FJ. Activated interstitial myofibroblasts express catabolic enzymes and mediate matrix remodeling in myxomatous heart valves. Circulation. 2001;104(21):2525–2532. - PubMed
-
- Tamura K, Fukuda Y, Ishizaki M, Masuda Y, Yamanaka N, Ferrans VJ. Abnormalities in elastic fibers and other connective-tissue components of floppy mitral valve. Am Heart J. 1995;129(6):1149–1158. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
