

The SCIentinel study--prospective multicenter study to define the spinal cord injury-induced immune depression syndrome (SCI-IDS)--study protocol and interim feasibility data
- PMID: 24206943
- PMCID: PMC3827331
- DOI: 10.1186/1471-2377-13-168
The SCIentinel study--prospective multicenter study to define the spinal cord injury-induced immune depression syndrome (SCI-IDS)--study protocol and interim feasibility data
Abstract
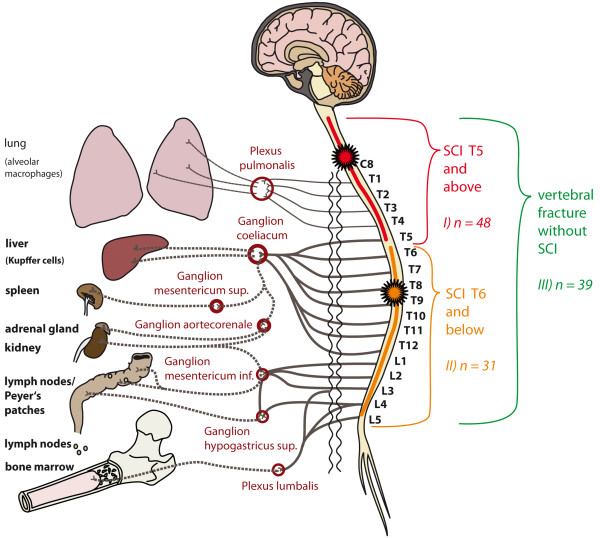
Background: Infections are the leading cause of death in the acute phase following spinal cord injury and qualify as independent risk factor for poor neurological outcome ("disease modifying factor"). The enhanced susceptibility for infections is not stringently explained by the increased risk of aspiration in tetraplegic patients, neurogenic bladder dysfunction, or by high-dose methylprednisolone treatment. Experimental and clinical pilot data suggest that spinal cord injury disrupts the balanced interplay between the central nervous system and the immune system. The primary hypothesis is that the Spinal Cord Injury-induced Immune Depression Syndrome (SCI-IDS) is 'neurogenic' including deactivation of adaptive and innate immunity with decreased HLA-DR expression on monocytes as a key surrogate parameter. Secondary hypotheses are that the Immune Depression Syndrome is i) injury level- and ii) severity-dependent, iii) triggers transient lymphopenia, and iv) causes qualitative functional leukocyte deficits, which may endure the post-acute phase after spinal cord injury.
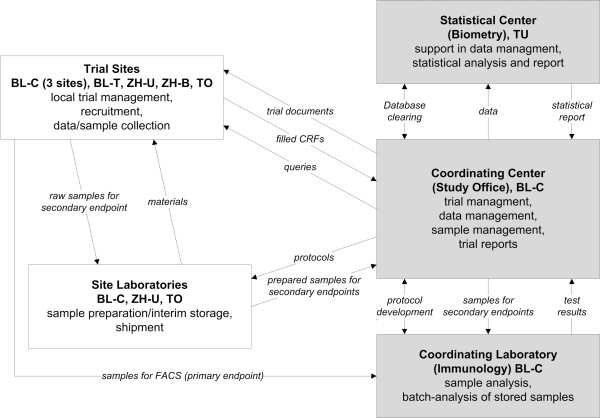
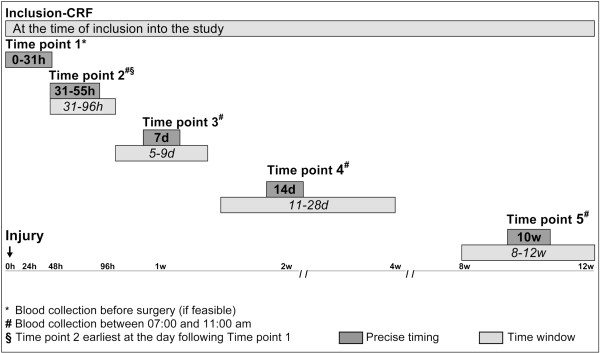
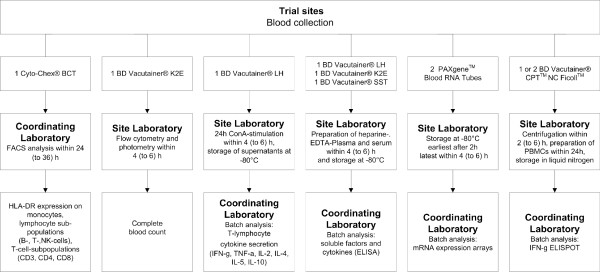
Methods/design: SCIentinel is a prospective, international, multicenter study aiming to recruit about 118 patients with acute spinal cord injury or control patients with acute vertebral fracture without neurological deficits scheduled for spinal surgery. The assessment points are: i) <31 hours, ii) 31-55 hours, iii) 7 days, iv) 14 days, and v) 10 weeks post-trauma. Assessment includes infections, concomitant injury, medication and neurological classification using American Spinal Injury Association impairment scale (AIS) and neurological level. Laboratory analyses comprise haematological profiling, immunophenotyping, including HLA-DR expression on monocytes, cytokines and gene expression of immune modulators. We provide an administrative interim analysis of the recruitment schedule of the trial.
Discussion: The objectives are to characterize the dysfunction of the innate and adaptive immune system after spinal cord injury and to explore its proposed 'neurogenic' origin by analyzing its correlation with lesion height and severity. The trial protocol considers difficulties of enrolment in an acute setting, and loss to follow up. The administrative interim analysis confirmed the feasibility of the protocol. Better understanding of the SCI-IDS is crucial to reduce co-morbidities and thereby to attenuate the impact of disease modifying factors to protect neurological "outcome at risk". This putatively results in improved spinal cord injury medical care.
Trial registration drks-id: DRKS00000122 (German Clinical Trials Registry).
Figures
References
-
- Meisel C, Schwab JM, Prass K, Meisel A, Dirnagl U. Central nervous system injury-induced immune deficiency syndrome. Nat Rev Neurosci. 2005;6(10):775–786. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
