

Diagnostic indicators of non-cardiovascular chest pain: a systematic review and meta-analysis
- PMID: 24207111
- PMCID: PMC4226211
- DOI: 10.1186/1741-7015-11-239
Diagnostic indicators of non-cardiovascular chest pain: a systematic review and meta-analysis
Abstract
Background: Non-cardiovascular chest pain (NCCP) has a high healthcare cost, but insufficient guidelines exist for its diagnostic investigation. The objective of the present work was to identify important diagnostic indicators and their accuracy for specific and non-specific conditions underlying NCCP.
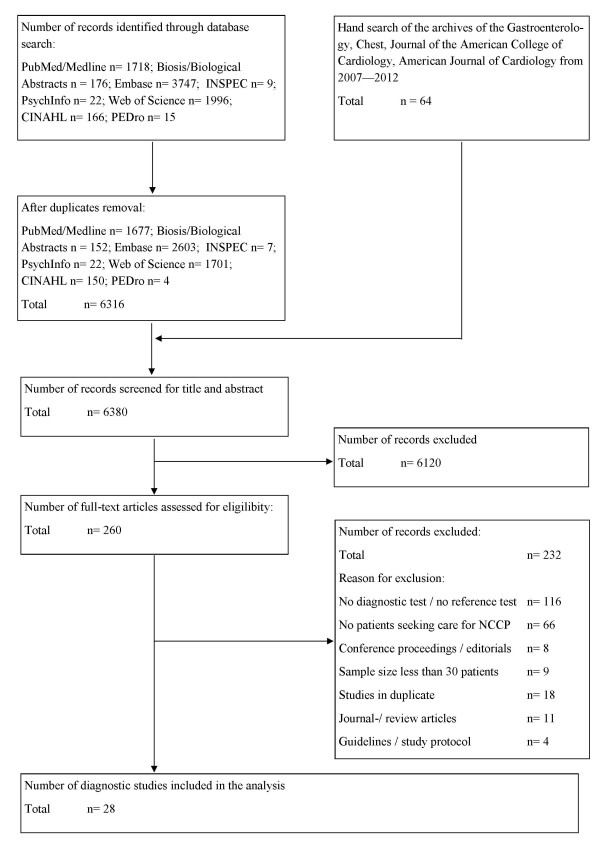
Methods: A systematic review and meta-analysis were performed. In May 2012, six databases were searched. Hand and bibliography searches were also conducted. Studies evaluating a diagnostic test against a reference test in patients with NCCP were included. Exclusion criteria were having <30 patients per group, and evaluating diagnostic tests for acute cardiovascular disease. Diagnostic accuracy is given in likelihood ratios (LR): very good (LR+ >10, LR- <0.1); good (LR + 5 to 10, LR- 0.1 to 0.2); fair (LR + 2 to 5, LR- 0.2 to 0.5); or poor (LR + 1 to 2, LR- 0.5 to 1). Joined meta-analysis of the diagnostic test sensitivity and specificity was performed by applying a hierarchical Bayesian model.
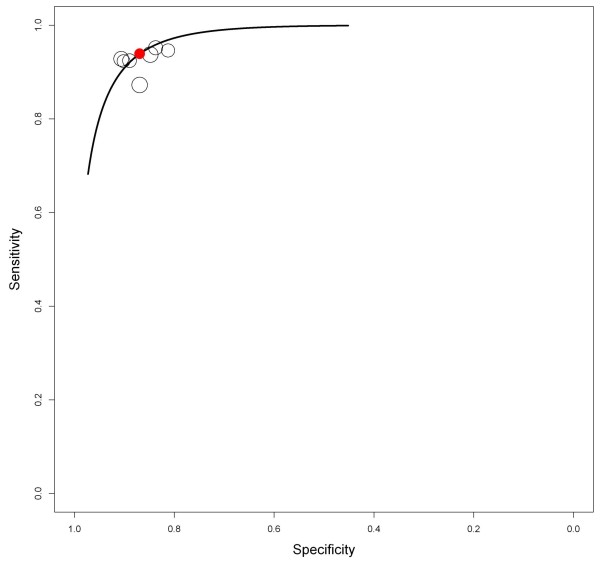
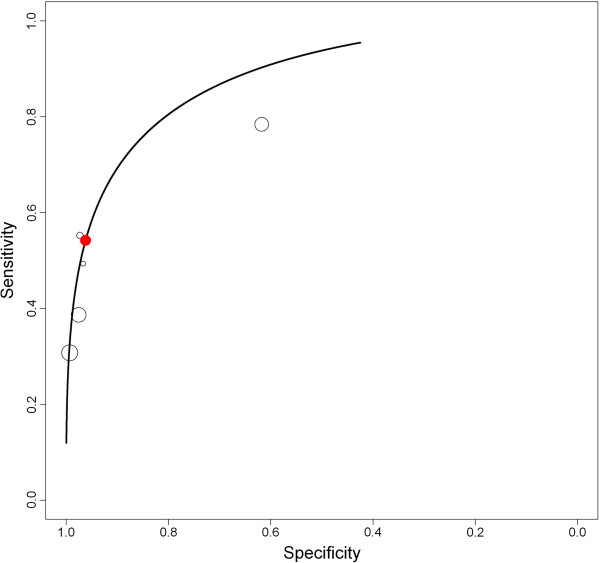
Results: Out of 6,316 records, 260 were reviewed in full text, and 28 were included: 20 investigating gastroesophageal reflux disorders (GERD), 3 musculoskeletal chest pain, and 5 psychiatric conditions. Study quality was good in 15 studies and moderate in 13. GERD diagnosis was more likely with typical GERD symptoms (LR + 2.70 and 2.75, LR- 0.42 and 0.78) than atypical GERD symptoms (LR + 0.49, LR- 2.71). GERD was also more likely with a positive response to a proton pump inhibitor (PPI) test (LR + 5.48, 7.13, and 8.56; LR- 0.24, 0.25, and 0.28); the posterior mean sensitivity and specificity of six studies were 0.89 (95% credible interval, 0.28 to 1) and 0.88 (95% credible interval, 0.26 to 1), respectively. Panic and anxiety screening scores can identify individuals requiring further testing for anxiety or panic disorders. Clinical findings in musculoskeletal pain either had a fair to moderate LR + and a poor LR- or vice versa.
Conclusions: In patients with NCCP, thorough clinical evaluation of the patient's history, symptoms, and clinical findings can indicate the most appropriate diagnostic tests. Treatment response to high-dose PPI treatment provides important information regarding GERD, and should be considered early. Panic and anxiety disorders are often undiagnosed and should be considered in the differential diagnosis of chest pain.
Figures
Similar articles
-
Treatment efficacy for non-cardiovascular chest pain: a systematic review and meta-analysis.PLoS One. 2014 Aug 11;9(8):e104722. doi: 10.1371/journal.pone.0104722. eCollection 2014. PLoS One. 2014. PMID: 25111147 Free PMC article.
-
Diagnostic test accuracy of nutritional tools used to identify undernutrition in patients with colorectal cancer: a systematic review.JBI Database System Rev Implement Rep. 2015 May 15;13(4):141-87. doi: 10.11124/jbisrir-2015-1673. JBI Database System Rev Implement Rep. 2015. PMID: 26447079
-
Signs and symptoms to determine if a patient presenting in primary care or hospital outpatient settings has COVID-19.Cochrane Database Syst Rev. 2022 May 20;5(5):CD013665. doi: 10.1002/14651858.CD013665.pub3. Cochrane Database Syst Rev. 2022. PMID: 35593186 Free PMC article.
-
Systematic review and modelling of the investigation of acute and chronic chest pain presenting in primary care.Health Technol Assess. 2004 Feb;8(2):iii, 1-158. doi: 10.3310/hta8020. Health Technol Assess. 2004. PMID: 14754562
-
Diagnostic tests and algorithms used in the investigation of haematuria: systematic reviews and economic evaluation.Health Technol Assess. 2006 Jun;10(18):iii-iv, xi-259. doi: 10.3310/hta10180. Health Technol Assess. 2006. PMID: 16729917
Cited by
-
Extra-Esophageal Presentation of Gastroesophageal Reflux Disease: 2020 Update.J Clin Med. 2020 Aug 7;9(8):2559. doi: 10.3390/jcm9082559. J Clin Med. 2020. PMID: 32784573 Free PMC article. Review.
-
Predicting coronary artery disease: a comparison between two data mining algorithms.BMC Public Health. 2019 Apr 29;19(1):448. doi: 10.1186/s12889-019-6721-5. BMC Public Health. 2019. PMID: 31035958 Free PMC article.
-
Rib Mediated Non-Cardiac Chest Pain: A Case Report.Cureus. 2020 Oct 6;12(10):e10831. doi: 10.7759/cureus.10831. Cureus. 2020. PMID: 33173637 Free PMC article.
-
Treatment efficacy for non-cardiovascular chest pain: a systematic review and meta-analysis.PLoS One. 2014 Aug 11;9(8):e104722. doi: 10.1371/journal.pone.0104722. eCollection 2014. PLoS One. 2014. PMID: 25111147 Free PMC article.
-
Prevalence and Overlap of Noncardiac Conditions in the Evaluation of Low-risk Acute Chest Pain Patients.Crit Pathw Cardiol. 2015 Sep;14(3):97-102. doi: 10.1097/HPC.0000000000000050. Crit Pathw Cardiol. 2015. PMID: 26214812 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
