

Implementing wait-time reductions under Ontario government benchmarks (Pay-for-Results): a Cluster Randomized Trial of the Effect of a Physician-Nurse Supplementary Triage Assistance team (MDRNSTAT) on emergency department patient wait times
- PMID: 24207160
- PMCID: PMC4225765
- DOI: 10.1186/1471-227X-13-17
Implementing wait-time reductions under Ontario government benchmarks (Pay-for-Results): a Cluster Randomized Trial of the Effect of a Physician-Nurse Supplementary Triage Assistance team (MDRNSTAT) on emergency department patient wait times
Abstract
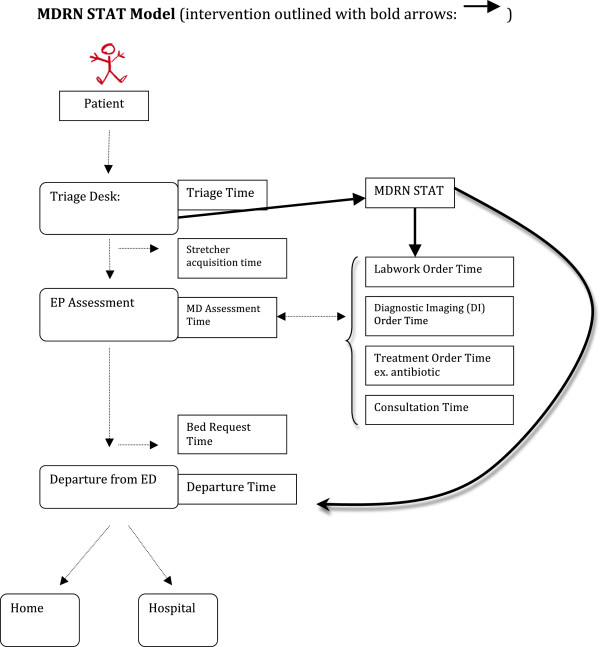
Background: Internationally, emergency departments are struggling with crowding and its associated morbidity, mortality, and decreased patient and health-care worker satisfaction. The objective was to evaluate the addition of a MDRNSTAT (Physician (MD)-Nurse (RN) Supplementary Team At Triage) on emergency department patient flow and quality of care.
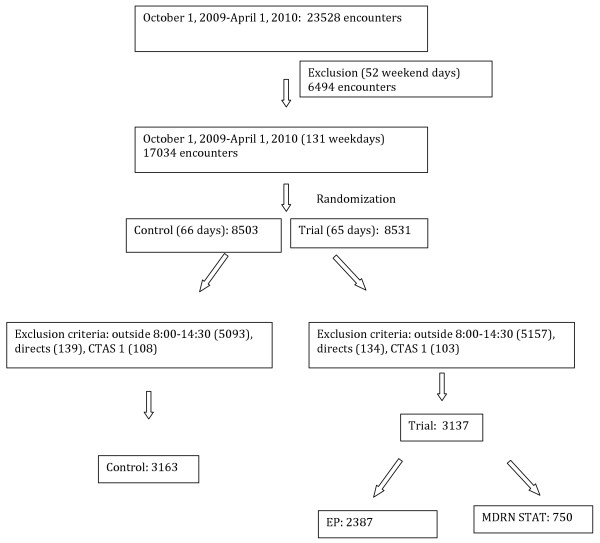
Methods: Pragmatic cluster randomized trial. From 131 weekday shifts (8:00-14:30) during a 26-week period, we randomized 65 days (3173 visits) to the intervention cluster with a MDRNSTAT presence, and 66 days (3163 visits) to the nurse-only triage control cluster. The primary outcome was emergency department length-of-stay (EDLOS) for patients managed and discharged only by the emergency department. Secondary outcomes included EDLOS for patients initially seen by the emergency department, and subsequently consulted and admitted, patients reaching government-mandated thresholds, time to initial physician assessment, left-without being seen rate, time to investigation, and measurement of harm.
Results: The intervention's median EDLOS for discharged, non-consulted, high acuity patients was 4:05 [95th% CI: 3:58 to 4:15] versus 4:29 [95th% CI: 4:19-4:38] during comparator shifts. The intervention's median EDLOS for discharged, non-consulted, low acuity patients was 1:55 [95th% CI: 1:48 to 2:05] versus 2:08 [95th% CI: 2:02-2:14]. The intervention's median physician initial assessment time was 0:55 [95th% CI: 0:53 to 0:58] versus 1:21 [95th% CI: 1:18 to 1:25]. The intervention's left-without-being-seen rate was 1.5% versus 2.2% for the control (p = 0.06). The MDRNSTAT subgroup analysis resulted in significant decreases in median EDLOS for discharged, non-consulted high (4:01 [95th% CI: 3:43-4:16]) and low acuity patients (1:10 95th% CI: 0:58-1:19]), as well as physician initial assessment time (0:25 [95th% CI: 0:23-0:26]). No patients returned to the emergency department after being discharged by the MDRNSTAT at triage.
Conclusions: The intervention reduced delays and left-without-being-seen rate without increased return visits or jeopardizing urgent care of severely ill patients.
Trial registration number: NCT00991471 ClinicalTrials.gov.
Figures
Similar articles
-
Cost-effectiveness of a physician-nurse supplementary triage assessment team at an academic tertiary care emergency department.CJEM. 2016 May;18(3):191-204. doi: 10.1017/cem.2015.88. Epub 2015 Sep 4. CJEM. 2016. PMID: 26337026 Clinical Trial.
-
Factors associated with failure of emergency wait-time targets for high acuity discharges and intensive care unit admissions.CJEM. 2018 Jan;20(1):112-124. doi: 10.1017/cem.2017.16. Epub 2017 May 18. CJEM. 2018. PMID: 28516829
-
Avoiding prolonged waiting time during busy periods in the emergency department: Is there a role for the senior emergency physician in triage?Eur J Emerg Med. 2006 Dec;13(6):342-8. doi: 10.1097/01.mej.0000224425.36444.50. Eur J Emerg Med. 2006. PMID: 17091056 Clinical Trial.
-
Effective strategies for reducing patient length of stay in the emergency department: a systematic review and meta-analysis.BMC Emerg Med. 2025 Feb 20;25(1):25. doi: 10.1186/s12873-024-01163-y. BMC Emerg Med. 2025. PMID: 39979831 Free PMC article.
-
Improving emergency department flow by introducing four interventions simultaneously. A quality improvement project.Int Emerg Nurs. 2024 Sep;76:101499. doi: 10.1016/j.ienj.2024.101499. Epub 2024 Aug 10. Int Emerg Nurs. 2024. PMID: 39128253 Review.
Cited by
-
Effectiveness of Resident Physicians as Triage Liaison Providers in an Academic Emergency Department.West J Emerg Med. 2017 Jun;18(4):577-584. doi: 10.5811/westjem.2017.1.33243. Epub 2017 Apr 17. West J Emerg Med. 2017. PMID: 28611876 Free PMC article.
-
Transitions of care for older adults discharged home from the emergency department: an inductive thematic content analysis of patient comments.BMC Geriatr. 2024 Jan 3;24(1):8. doi: 10.1186/s12877-023-04482-0. BMC Geriatr. 2024. PMID: 38172725 Free PMC article.
-
Replication of an emergency department-based recovery coaching intervention and pilot testing of pragmatic trial protocols within the context of Indiana's Opioid State Targeted Response plan.J Subst Abuse Treat. 2020 Jan;108:88-94. doi: 10.1016/j.jsat.2019.06.002. Epub 2019 Jun 6. J Subst Abuse Treat. 2020. PMID: 31200985 Free PMC article. Clinical Trial.
-
Emergency department utilization, admissions, and revisits in the United States (New York), Canada (Ontario), and New Zealand: A retrospective cross-sectional analysis.Acad Emerg Med. 2023 Sep;30(9):946-954. doi: 10.1111/acem.14738. Epub 2023 May 8. Acad Emerg Med. 2023. PMID: 37062045 Free PMC article.
-
Efficiency measures of emergency departments: an Italian systematic literature review.BMJ Open Qual. 2021 Sep;10(3):e001058. doi: 10.1136/bmjoq-2020-001058. BMJ Open Qual. 2021. PMID: 34493488 Free PMC article.
References
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
