

Early time-limited antiretroviral therapy versus deferred therapy in South African infants infected with HIV: results from the children with HIV early antiretroviral (CHER) randomised trial
- PMID: 24209829
- PMCID: PMC4104982
- DOI: 10.1016/S0140-6736(13)61409-9
Early time-limited antiretroviral therapy versus deferred therapy in South African infants infected with HIV: results from the children with HIV early antiretroviral (CHER) randomised trial
Abstract
Background: Interim results from the children with HIV early antiretroviral (CHER) trial showed that early antiretroviral therapy (ART) was life-saving for infants infected with HIV. In view of the few treatment options and the potential toxicity associated with lifelong ART, in the CHER trial we compared early time-limited ART with deferred ART.
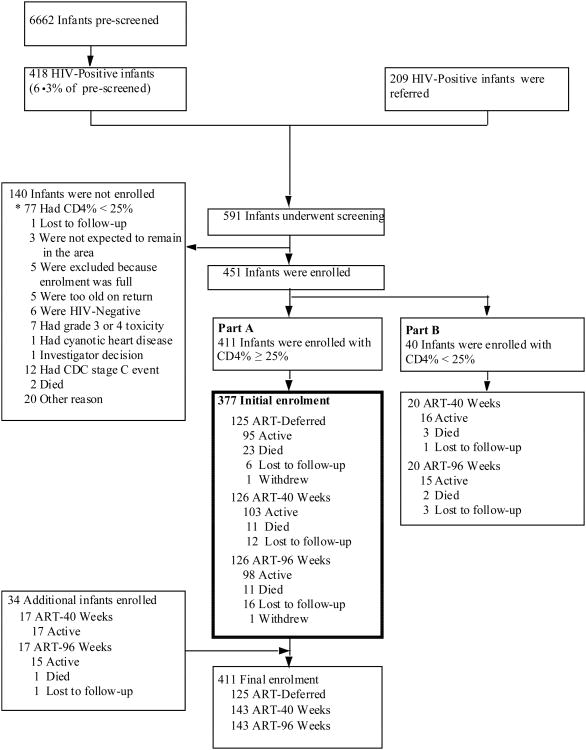
Methods: CHER was an open-label randomised controlled trial of HIV-infected asymptomatic infants younger than 12 weeks in two South African trial sites with a percentage of CD4-positive T lymphocytes (CD4%) of 25% or higher. 377 infants were randomly allocated to one of three groups: deferred ART (ART-Def), immediate ART for 40 weeks (ART-40W), or immediate ART for 96 weeks (ART-96W), with subsequent treatment interruption. The randomisation schedule was stratified by clinical site with permuted blocks of random sizes to balance the numbers of infants allocated to each group. Criteria for ART initiation in the ART-Def group and re-initiation after interruption in the other groups were CD4% less than 25% in infancy; otherwise, the criteria were CD4% less than 20% or Centers for Disease Control and Prevention severe stage B or stage C disease. Combination therapy of lopinavir-ritonavir, zidovudine, and lamivudine was the first-line treatment regimen at ART initiation and re-initiation. The primary endpoint was time to failure of first-line ART (immunological, clinical, or virological) or death. Comparisons were done by intention-to-treat analysis, with use of time-to-event methods. This trial is registered with ClinicalTrials.gov, number NCT00102960.
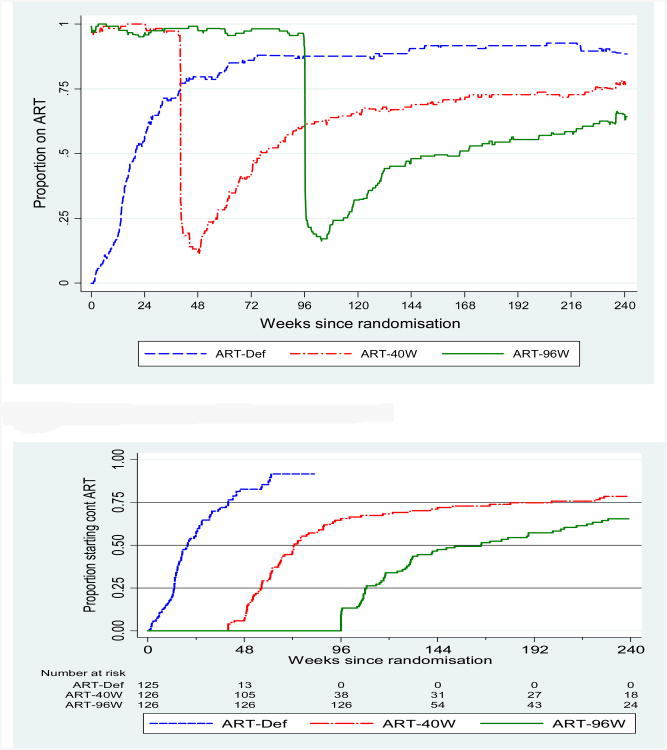
Findings: 377 infants were enrolled, with a median age of 7·4 weeks, CD4% of 35%, and HIV RNA log 5·7 copies per mL. Median follow-up was 4·8 years; 34 infants (9%) were lost to follow-up. Median time to ART initiation in the ART-Def group was 20 weeks (IQR 16-25). Time to restarting of ART after interruption was 33 weeks (26-45) in ART-40W and 70 weeks (35-109) in ART-96W; at the end of the trial, 19% of patients in ART-40W and 32% of patients in ART-96W remained off ART. Proportions of follow-up time spent on ART were 81% in the ART-Def group, 70% in the ART-40W group, and 69% in the ART-96W group. 48 (38%) of 125 children in the ART-Def group, 32 (25%) of 126 in the ART-40W group, and 26 (21%) of 126 in the ART-96W group reached the primary endpoint. The hazard ratio, relative to ART-Def, was 0·59 (95% CI 0·38-0·93, p=0·02) for ART-40W and 0·47 (0·27-0·76, p=0·002) for ART-96W. Three children in ART-Def, three in ART-40W, and one in ART-96W switched to second-line ART.
Interpretation: Early time-limited ART had better clinical and immunological outcomes than deferred ART, with no evidence of excess disease progression during subsequent treatment interruption and less overall ART exposure than deferred ART. Longer time on primary ART permits longer subsequent interruption, with marginally better outcomes.
Funding: US National Institutes of Health.
Copyright © 2013 Elsevier Ltd. All rights reserved.
Figures
Comment in
-
Does the CHER trial open up new therapeutic perspectives?Lancet. 2013 Nov 9;382(9904):1539-40. doi: 10.1016/S0140-6736(13)61717-1. Lancet. 2013. PMID: 24209812 No abstract available.
References
-
- Bourne DE, Thompson M, Brody LL, et al. Emergence of a peak in early infant mortality due to HIV/AIDS in South Africa. AIDS. 2009;23(1):101–6. - PubMed
-
- Marinda E, Humphrey JH, Iliff PJ, et al. Child mortality according to maternal and infant HIV status in Zimbabwe. Pediatr Infect Dis J. 2007;26(6):519–26. - PubMed
-
- Newell ML, Coovadia H, Cortina-Borja M, Rollins N, Gaillard P, Dabis F. Mortality of infected and uninfected infants born to HIV-infected mothers in Africa: a pooled analysis. Lancet. 2004;364(9441):1236–43. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
