

Inactivated autograft-prosthesis composite has a role for grade III giant cell tumor of bone around the knee
- PMID: 24209887
- PMCID: PMC4225750
- DOI: 10.1186/1471-2474-14-319
Inactivated autograft-prosthesis composite has a role for grade III giant cell tumor of bone around the knee
Abstract
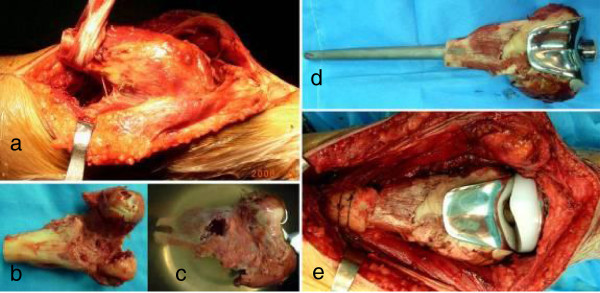
Background: Giant cell tumors (GCT) around the knee are common and pose a special problem of reconstruction after tumor excision, especially for grade III GCT. We questioned whether en bloc resection and reconstruction with alcohol inactivated autograft-prosthesis composite would provide (1) local control and long-term survival and (2) useful limb function in patients who had grade III GCT around the knee.
Methods: We retrospectively reviewed eight patients (5 males and 3 females) treated with this procedure with mean age of 31 years (range 20 to 43 years) from Jan 2007 to Oct 2008. 5 lesions were located in distal femur and 3 in proximal tibia. 4 patients were with primary tumor and the other 4 with recurrence. 2 patients showed pathological fracture.
Results: Mean Follow-up is 54 months ranging from 38 to 47 months. No recurrence, metastasis, prosthesis loosening were found. The mean healing time between autograft and host bone was 5.5 months. The mean MSTS score was 26.3 (88%) ranging from 25 to 29. The mean ISOLS composite graft score was 32.8 (88.5%) ranging from 28 to 35. Creeping substitution is possibly the main way in bony junction. The healing time in femoral lesion is faster than that in tibial lesion.
Conclusions: The technique of alcohol inactivated autograft-prosthesis composite could be able to achieve satisfactory oncological and functional outcomes in Grade III GCT.
Figures


Similar articles
-
Long-term outcome of giant cell tumors of bone around the knee treated by en bloc resection of tumor and reconstruction with prosthesis.Orthop Surg. 2010 Aug;2(3):211-7. doi: 10.1111/j.1757-7861.2010.00089.x. Orthop Surg. 2010. PMID: 22009951 Free PMC article.
-
Factors of local recurrence of giant cell tumor of long bone after treatment: plain radiographs, pathology and surgical procedures.J Med Assoc Thai. 2011 Oct;94(10):1230-7. J Med Assoc Thai. 2011. PMID: 22145509
-
Clinical and Radiographic Results of Reconstruction with Fibular Autograft for Distal Radius Giant Cell Tumor.Orthop Surg. 2016 May;8(2):196-204. doi: 10.1111/os.12242. Orthop Surg. 2016. PMID: 27384728 Free PMC article.
-
Reconstruction with Custom Unicondylar Hemiarthroplasty following Tumor Resection: A Case Series and Review of the Literature.J Knee Surg. 2020 Aug;33(8):818-824. doi: 10.1055/s-0039-1688556. Epub 2019 May 8. J Knee Surg. 2020. PMID: 31067588 Review.
-
De novo malignant transformation of giant cell tumor of bone.Skeletal Radiol. 2001 Feb;30(2):104-8. doi: 10.1007/s002560000305. Skeletal Radiol. 2001. PMID: 11310196 Review.
Cited by
-
The long-term outcomes following the use of inactivated autograft in the treatment of primary malignant musculoskeletal tumor.J Orthop Surg Res. 2015 Nov 17;10:177. doi: 10.1186/s13018-015-0324-3. J Orthop Surg Res. 2015. PMID: 26577680 Free PMC article.
-
Comparative efficacy of intraoperative extracorporeal irradiated and alcohol-inactivated autograft reimplantation for the management of osteosarcomas-a multicentre retrospective study.World J Surg Oncol. 2021 May 26;19(1):157. doi: 10.1186/s12957-021-02271-w. World J Surg Oncol. 2021. PMID: 34039361 Free PMC article.
-
Limb function and quality of life after various reconstruction methods according to tumor location following resection of osteosarcoma in distal femur.BMC Musculoskelet Disord. 2014 Dec 23;15:453. doi: 10.1186/1471-2474-15-453. BMC Musculoskelet Disord. 2014. PMID: 25539904 Free PMC article.
-
Impacts of Tumor Location, Nature and Bone Destruction of Extremity Osteosarcoma on Selection of Limb Salvage Operative Procedure.Orthop Surg. 2016 May;8(2):139-49. doi: 10.1111/os.12237. Orthop Surg. 2016. PMID: 27384722 Free PMC article.
-
Use of three-dimensional-printed custom-made prosthesis to treat unicondylar femoral defect secondary to pathological fracture caused by giant cell tumor.J Int Med Res. 2021 Jul;49(7):3000605211025347. doi: 10.1177/03000605211025347. J Int Med Res. 2021. PMID: 34212773 Free PMC article.
References
-
- Ghert MA, Rizzo M, Harrelson JM. et al.Giant-cell tumor of the appendicular skeleton. Clin Orthop Relat Res. 2002;400:201–210. - PubMed
-
- Prosser GH, Baloch KG, Tillman RM. et al.Does curettage without adjuvant therapy provide low recurrence rates in giant-cell tumors of bone? Clin Orthop Relat Res. 2005;435:211–218. - PubMed
-
- Lackman RD, Hosalkar HS, Ogilvie CM. Intralesional curettage for grades II and III giant cell tumors of bone. Clin Orthop Relat Res. 2005;438:123–127. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
