

doi: 10.1016/j.hcl.2013.08.009.
Pediatric hand fractures
Affiliations
- PMID: 24209954
- PMCID: PMC4153349
- DOI: 10.1016/j.hcl.2013.08.009
Item in Clipboard
Pediatric hand fractures
Hand Clin.
2013 Nov.
Abstract
Pediatric hand fractures are common childhood injuries. Identification of the fractures in the emergency room setting can be challenging owing to the physes and incomplete ossification of the carpus that are not revealed in the radiographs. Most simple fractures can be treated with appropriate immobilization through buddy taping, finger splints, or casting. If correctly diagnosed, reduced, and immobilized, these fractures usually result in excellent clinical outcomes.
Keywords: Malunion; Pediatric hand fractures; Physeal injuries of the hand; Radiographs.
Copyright © 2013 Elsevier Inc. All rights reserved.
Figures

This late presentation of a dorsally displaced and shortened P1 fracture in 11 year-old girl demonstrates extensive remodeling in the sagittal plane over 2 years.

Six year-old boy with middle and ring fingertip crush injury and a closed subungal hematoma on the ring finger. The fractures persisted on x-ray 5 months after injury.

Innocuous clinical presentation of a Seymour fracture with an open physeal fracture identified on true lateral xray. Note that the lunula appears much larger than any of the other nails, indicating the nail is avulsed from the nail bed and sitting atop the eponychial fold.
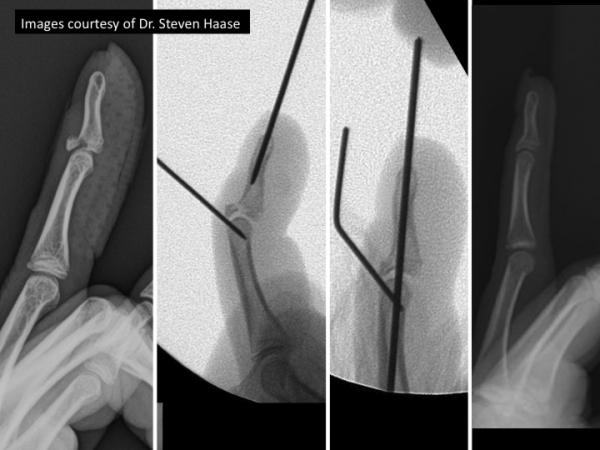
Fixation of an adolescent bony mallet fracture using ishiguro extendion block technique

Two year-old girl with an unwitnessed injury to her left index finger. She presented 10 months later with an intracondylar proximal phalanx malunion. Due to persistent deformity and inability to form a closed fist, she underwent a corrective osteotomy 8 years later with good final results despite the known risk of AVN.

Two year-old girl with an unwitnessed injury to her left index finger. She presented 10 months later with an intracondylar proximal phalanx malunion. Due to persistent deformity and inability to form a closed fist, she underwent a corrective osteotomy 8 years later with good final results despite the known risk of AVN.

Three year-old girl presented two weeks after right small finger injury. Xrays show a small finger distal condylar phalangeal (DCP) fracture, with no bony contact (Type III). Despite efforts to reduce and stabilize the fracture, the fracture went on to a non-union with minimal motion at the PIP joint.
References
-
- Landin LA. Epidemiology of children's fractures. J of Pediatric Orthopaedics. 1997;6(2):79–83. - PubMed
-
- Worlock P, Stower M. Fracture patterns in Nottingham children. J of Pediatric Orthopedics. 1986;6(6):656–660. - PubMed
-
- Worlock P, Stower M. The incidence and pattern of hand fractures in children. J of Hand Surg (Br) 1986;11(2):198–200. - PubMed
-
- Vadivelu R, Dias JJ, Burke FD, Stanton J. Hand injuries in children: a prospective study. J Ped Orthopedics. 2006;26(1):29–35. - PubMed
-
- Chung KC, Spilson SV. The frequency and epidemiology of hand and forearm fractures in the United States. J Hand Surg (Am) 2001;26(5):908–915. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
