

External beam radiotherapy of recurrent glioma: radiation tolerance of the human brain
- PMID: 24213316
- PMCID: PMC3712703
- DOI: 10.3390/cancers4020379
External beam radiotherapy of recurrent glioma: radiation tolerance of the human brain
Abstract
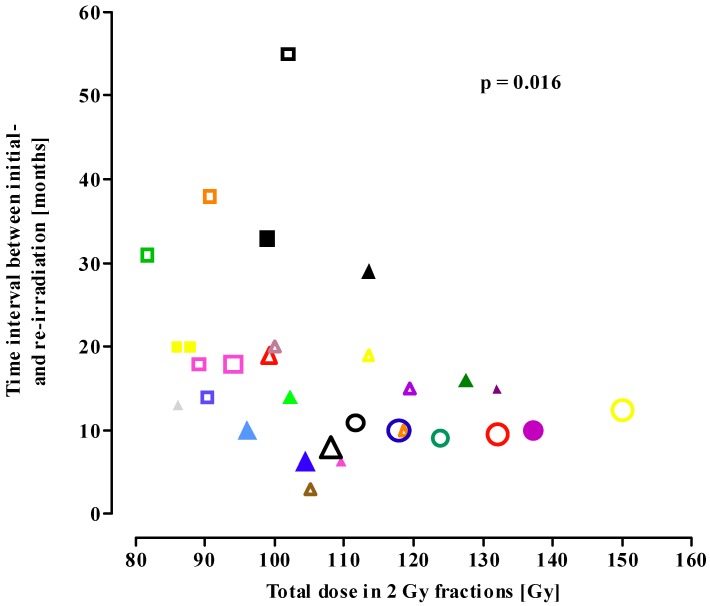
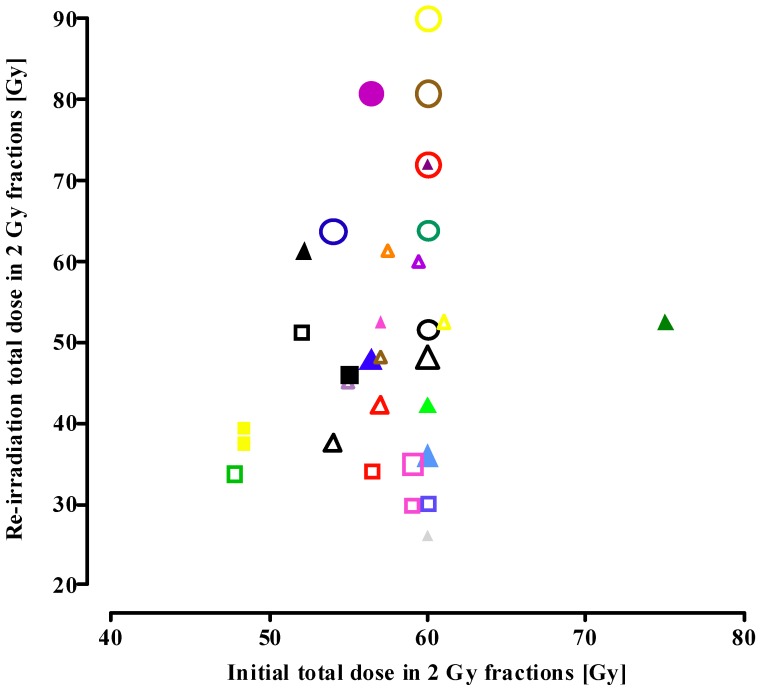
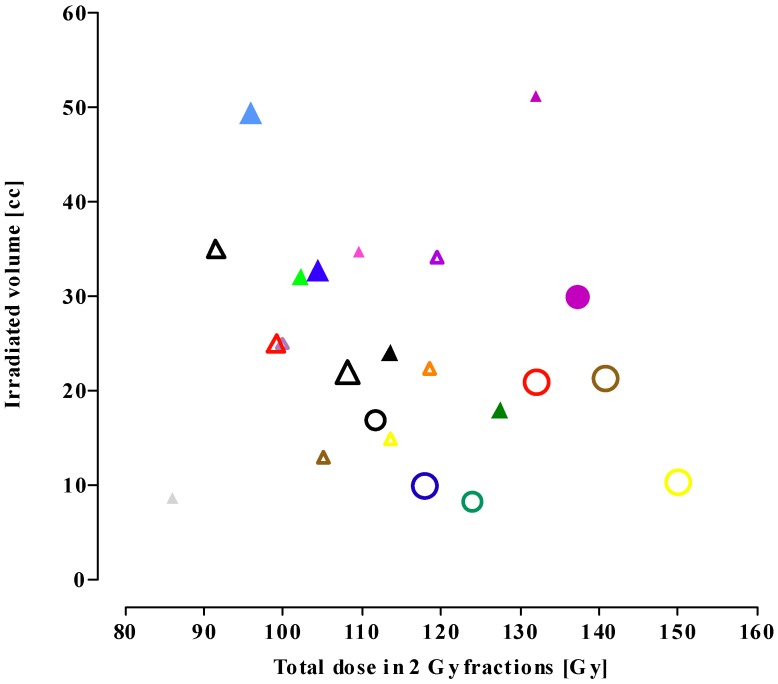
Malignant gliomas relapse in close proximity to the resection site, which is the postoperatively irradiated volume. Studies on re-irradiation of glioma were examined regarding radiation-induced late adverse effects (i.e., brain tissue necrosis), to obtain information on the tolerance dose and treatment volume of normal human brain tissue. The studies were analyzed using the linear-quadratic model to express the re-irradiation tolerance in cumulative equivalent total doses when applied in 2 Gy fractions (EQD2cumulative). Analysis shows that the EQD2cumulative increases from conventional re-irradiation series to fractionated stereotactic radiotherapy (FSRT) to LINAC-based stereotactic radiosurgery (SRS). The mean time interval between primary radiotherapy and the re-irradiation course was shortened from 30 months for conventional re-irradiation to 17 and 10 months for FSRT and SRS, respectively. Following conventional re-irradiation, radiation-induced normal brain tissue necrosis occurred beyond an EQD2cumulative around 100 Gy. With increasing conformality of therapy, the smaller the treatment volume is, the higher the radiation dose that can be tolerated. Despite the dose escalation, no increase in late normal tissue toxicity was reported. On basis of our analysis, the use of particle therapy in the treatment of recurrent gliomas, because of the optimized physical dose distribution in the tumour and surrounding healthy brain tissue, should be considered for future clinical trials.
Figures
References
-
- Stupp R., Mason W.P., van den Bent M.J., Weller M., Fisher B., Taphoorn M.J., Belanger K., Brandes A.A., Marosi C., Bogdahn U., et al. Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. N. Engl. J. Med. 2005;352:987–996. - PubMed
-
- Stupp R., Hegi M.E., Mason W.P., van den Bent M.J., Taphoorn M.J., Janzer R.C., Ludwin S.K., Allgeier A., Fisher B., Belanger K., et al. Effects of radiotherapy with concomitant and adjuvant temozolomide versus radiotherapy alone on survival in glioblastoma in a randomised phase III study: 5-Year analysis of the EORTC-NCIC trial. Lancet Oncol. 2009;10:459–466. - PubMed
-
- Jansen E.P., Dewit L.G., van Herk M., Bartelink H. Target volumes in radiotherapy for high grade malignant glioma of the brain. Radiother. Oncol. 2000;56:151–156. - PubMed
-
- Emami B., Lyman J., Brown A., Coia L., Goitein M., Munzenrider J.E., Shank B., Solin L.J., Wesson M. Tolerance of normal tissue to therapeutic irradiation. Int. J. Radiat. Oncol. Biol. Phys. 1991;21:109–122. - PubMed
LinkOut - more resources
Full Text Sources
