

Non-invasive ventilation for acute hypoxemic respiratory failure: intubation rate and risk factors
- PMID: 24215648
- PMCID: PMC4057073
- DOI: 10.1186/cc13103
Non-invasive ventilation for acute hypoxemic respiratory failure: intubation rate and risk factors
Abstract
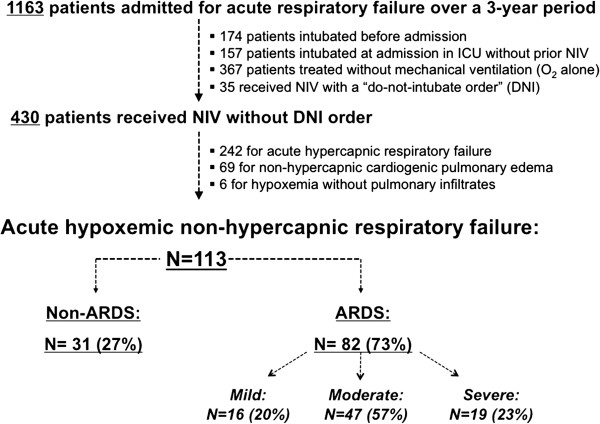
Introduction: We assessed rates and predictive factors of non-invasive ventilation (NIV) failure in patients admitted to the intensive care unit (ICU) for non-hypercapnic acute hypoxemic respiratory failure (AHRF).
Methods: This is an observational cohort study using data prospectively collected over a three-year period in a medical ICU of a university hospital.
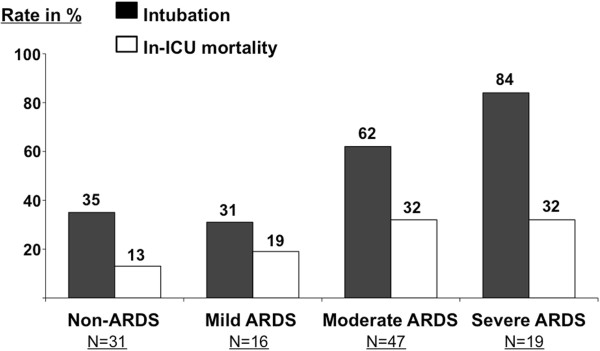
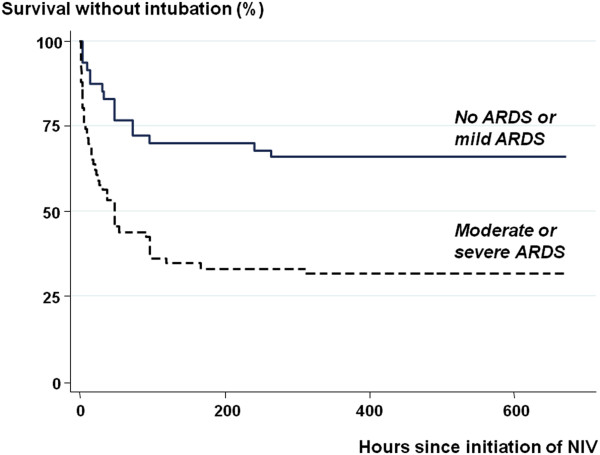
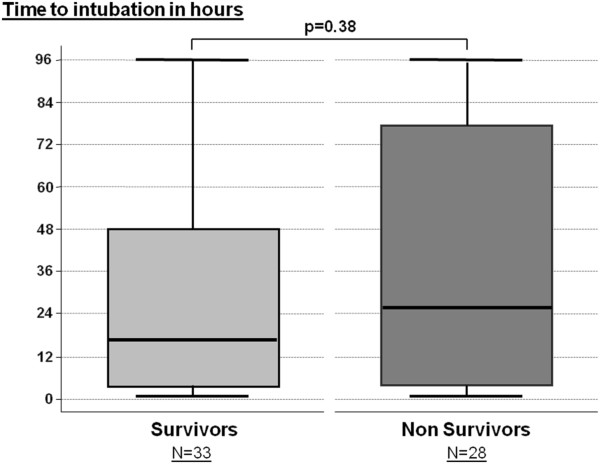
Results: Among 113 patients receiving NIV for AHRF, 82 had acute respiratory distress syndrome (ARDS) and 31 had non-ARDS. Intubation rates significantly differed between ARDS and non-ARDS patients (61% versus 35%, P = 0.015) and according to clinical severity of ARDS: 31% in mild, 62% in moderate, and 84% in severe ARDS (P = 0.0016). In-ICU mortality rates were 13% in non-ARDS, and, respectively, 19%, 32% and 32% in mild, moderate and severe ARDS (P = 0.22). Among patients with moderate ARDS, NIV failure was lower among those having a PaO2/FiO2 >150 mmHg (45% vs. 74%, p = 0.04). NIV failure was associated with active cancer, shock, moderate/severe ARDS, lower Glasgow coma score and lower positive end-expiratory pressure level at NIV initiation. Among intubated patients, ICU mortality rate was 46% overall and did not differ according to the time to intubation.
Conclusions: With intubation rates below 35% in non-ARDS and mild ARDS, NIV stands as the first-line approach; NIV may be attempted in ARDS patients with a PaO2/FiO2 > 150. By contrast, 84% of severe ARDS required intubation and NIV did not appear beneficial in this subset of patients. However, the time to intubation had no influence on mortality.
Figures

References
-
- Lightowler JV, Wedzicha JA, Elliott MW, Ram FS. Non-invasive positive pressure ventilation to treat respiratory failure resulting from exacerbations of chronic obstructive pulmonary disease: Cochrane systematic review and meta-analysis. BMJ. 2003;17:185. doi: 10.1136/bmj.326.7382.185. - DOI - PMC - PubMed
-
- Keenan SP, Sinuff T, Cook DJ, Hill NS. Which patients with acute exacerbation of chronic obstructive pulmonary disease benefit from noninvasive positive-pressure ventilation? A systematic review of the literature. Ann Intern Med. 2003;17:861–870. doi: 10.7326/0003-4819-138-11-200306030-00007. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
