

Resuscitation of preterm neonates with limited versus high oxygen strategy
- PMID: 24218465
- PMCID: PMC3838529
- DOI: 10.1542/peds.2013-0978
Resuscitation of preterm neonates with limited versus high oxygen strategy
Abstract
Objective: To determine whether a limited oxygen strategy (LOX) versus a high oxygen strategy (HOX) during delivery room resuscitation decreases oxidative stress in preterm neonates.
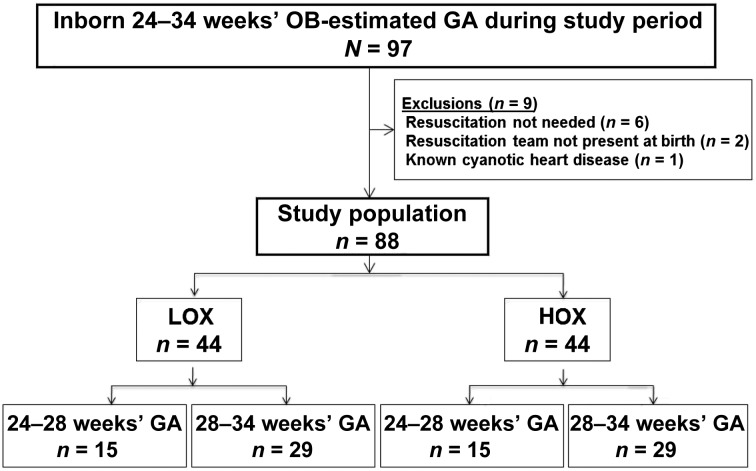
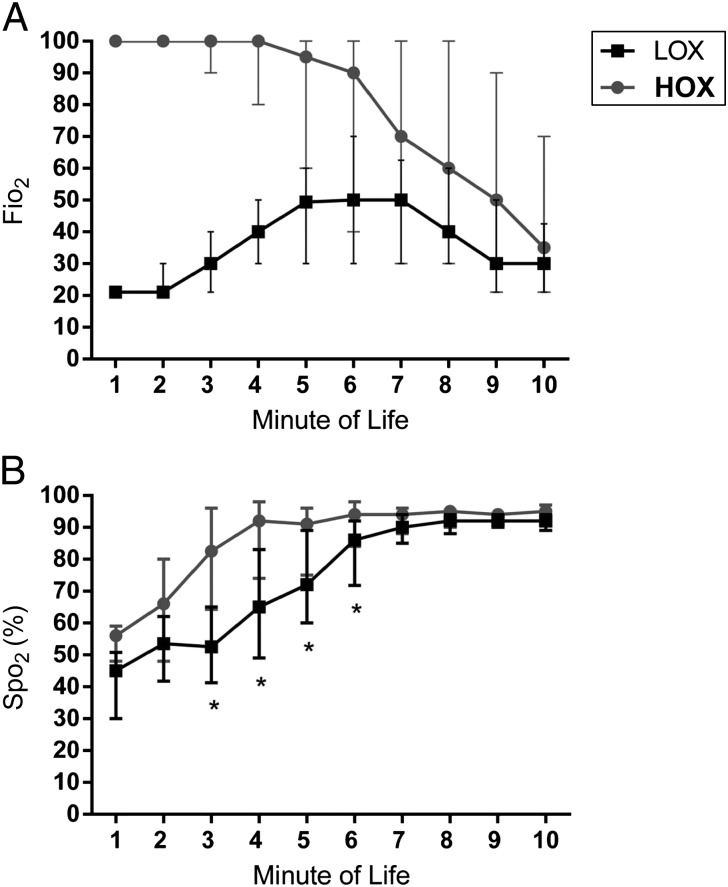
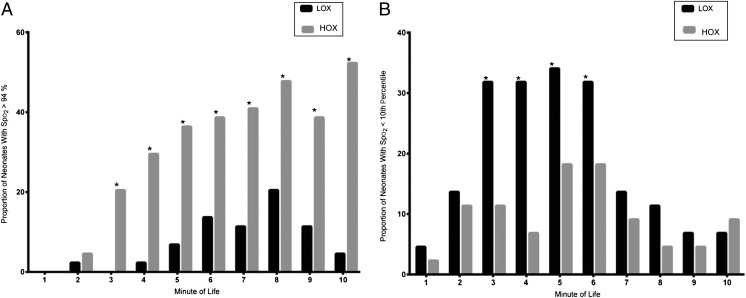
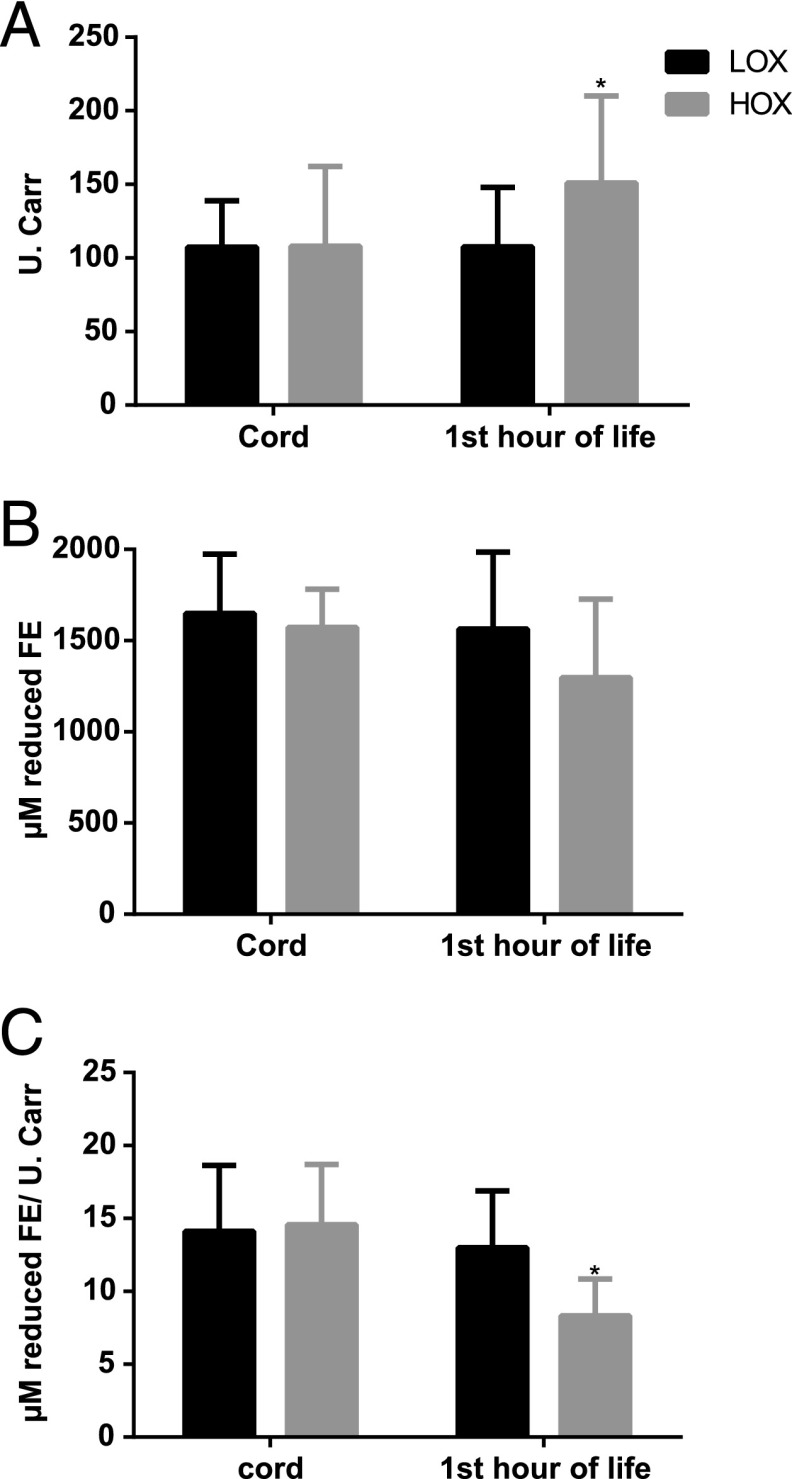
Methods: A randomized trial of neonates of 24 to 34 weeks' gestational age (GA) who received resuscitation was performed. LOX neonates received room air as the initial resuscitation gas, and fraction of inspired oxygen (Fio2) was adjusted by 10% every 30 seconds to achieve target preductal oxygen saturations (Spo2) as described by the 2010 Neonatal Resuscitation Program guidelines. HOX neonates received 100% O2 as initial resuscitation gas, and Fio2 was adjusted by 10% to keep preductal Spo2 at 85% to 94%. Total hydroperoxide (TH), biological antioxidant potential (BAP), and the oxidative balance ratio (BAP/TH) were analyzed in cord blood and the first hour of life. Secondary outcomes included delivery room interventions, respiratory support on NICU admission, and short-term morbidities.
Results: Forty-four LOX (GA: 30 ± 3 weeks; birth weight: 1678 ± 634 g) and 44 HOX (GA: 30 ± 3 weeks; birth weight: 1463 ± 606 g) neonates were included. LOX decreased integrated excess oxygen (∑Fio2 × time [min]) in the delivery room compared with HOX (401 ± 151 vs 662 ± 249; P < .01). At 1 hour of life, BAP/TH was 60% higher for LOX versus HOX neonates (13 [9-16] vs 8 [6-9]) µM/U.CARR, P < .01). LOX decreased ventilator days (3 [0-64] vs 8 [0-96]; P < .05) and reduced the incidence of bronchopulmonary dysplasia (7% vs 25%; P < .05).
Conclusions: LOX is feasible and results in less oxygen exposure, lower oxidative stress, and decreased respiratory morbidities and thus is a reasonable alternative for resuscitation of preterm neonates in the delivery room.
Trial registration: ClinicalTrials.gov NCT01697904.
Keywords: newborn; oxidative stress; oxygen; preterm; resuscitation.
Figures
Comment in
-
SUPPORTing premature infants.Pediatrics. 2013 Dec;132(6):e1661-3. doi: 10.1542/peds.2013-1292. Epub 2013 Nov 11. Pediatrics. 2013. PMID: 24218459 Free PMC article. No abstract available.
References
-
- Welty SE, Smith CV. Rationale for antioxidant therapy in premature infants to prevent bronchopulmonary dysplasia. Nutr Rev. 2001;59(1 pt 1):10–17 - PubMed
-
- Vento M, Escobar J, Cernada M, Escrig R, Aguar M. The use and misuse of oxygen during the neonatal period. Clin Perinatol. 2012;39(1):165–176 - PubMed
-
- Jobe AH, Bancalari E. Bronchopulmonary dysplasia. Am J Respir Crit Care Med. 2001;163(7):1723–1729 - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
