

Tumor-reactive CD8+ T cells in metastatic gastrointestinal cancer refractory to chemotherapy
- PMID: 24218514
- PMCID: PMC3927404
- DOI: 10.1158/1078-0432.CCR-13-1736
Tumor-reactive CD8+ T cells in metastatic gastrointestinal cancer refractory to chemotherapy
Abstract
Purpose: To evaluate whether patients with metastatic gastrointestinal adenocarcinomas refractory to chemotherapy harbor tumor-reactive cytotoxic T cells.
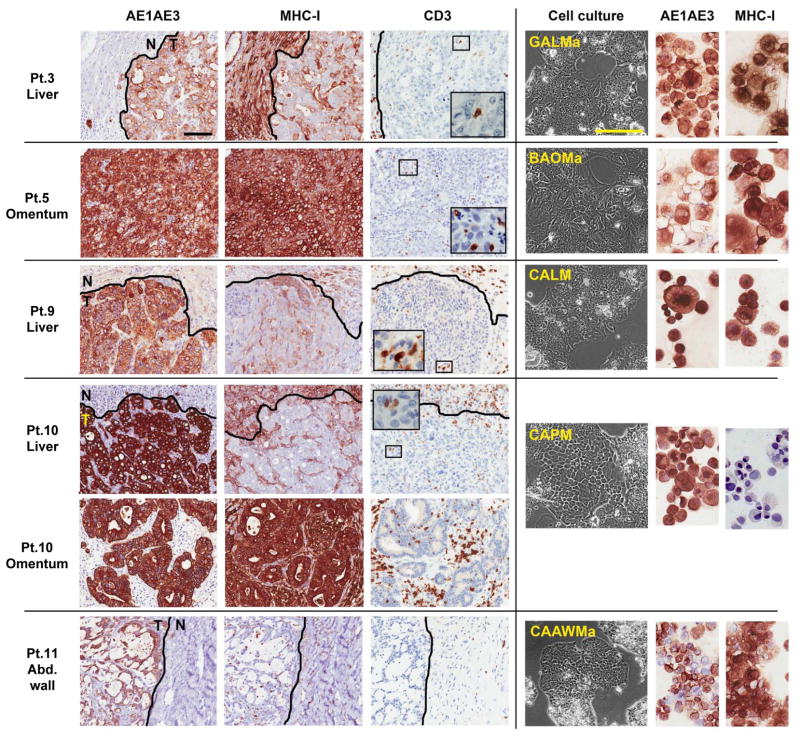
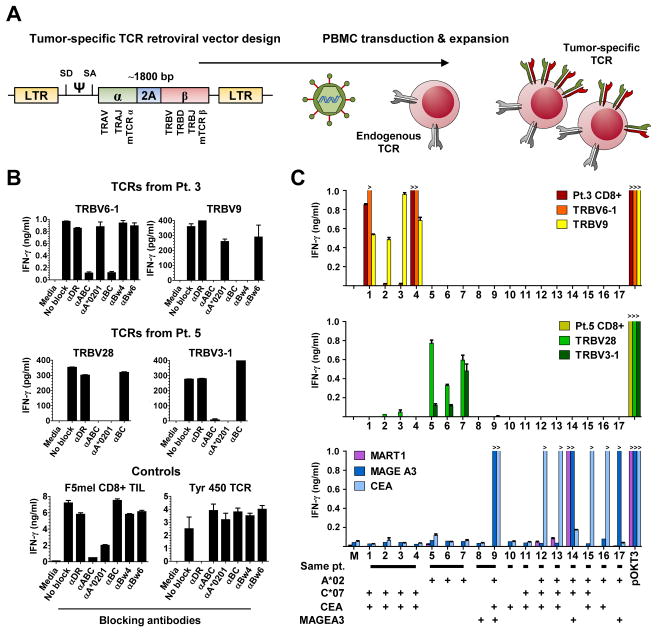
Experimental design: Expansion of CD8(+) tumor-infiltrating lymphocytes (TIL) and cancer cell lines was attempted from gastrointestinal cancer metastases in 16 consecutive patients for the study of antitumor immune recognition. Retroviral transduction of genes encoding T-cell receptors (TCR) was used to define HLA-restriction elements and specific reactivity.
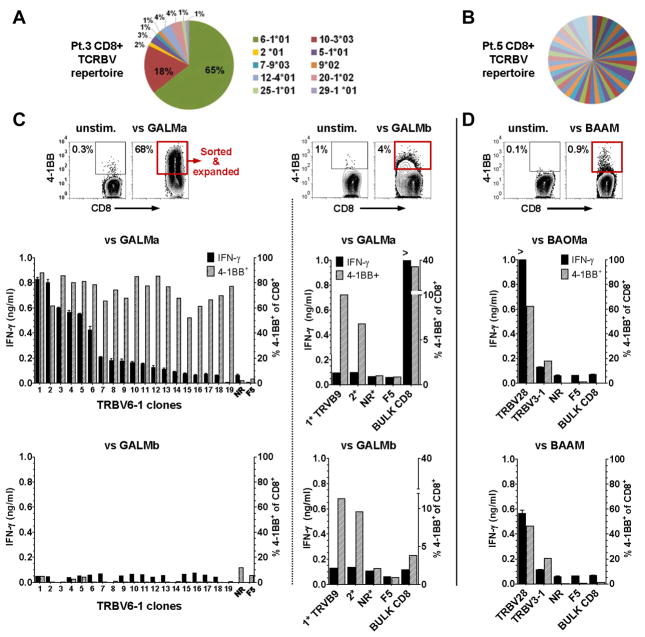
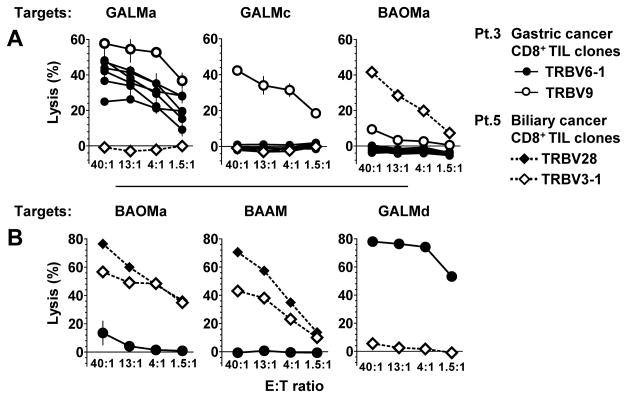
Results: TIL were expanded from metastases in all patients, and new tumor cell lines were generated in 5 patients. Autologous tumor recognition without cross-reactivity against allogeneic HLA-matched gastrointestinal tumors was found in CD8(+) TIL from 3 of these 5 patients. In a patient with gastric cancer liver metastases, the repertoire of CD8(+) TIL was dominated by cytolytic sister clones reactive to 2 out of 4 autologous cancer cell lines restricted by HLA-C*0701. From the same patient, a rare CD8(+) TIL clone with a distinct TCR recognized all four cancer cell lines restricted by HLA-B*4901. In a patient with bile duct cancer, two distinct antitumor cytolytic clones were isolated from a highly polyclonal CD8(+) TIL repertoire. TCRs isolated from these clones recognized epitopes restricted by HLA-A*0201. In a third patient, CD8(+) TIL reactivity was progressively lost against an autologous colon cancer cell line that displayed loss of HLA haplotype.
Conclusions: This study provides a basis for the development of immunotherapy for patients with advanced gastrointestinal malignancies by first establishing the presence of naturally occurring tumor-reactive CD8(+) TIL at the molecular level.
©2013 AACR.
Conflict of interest statement
Figures
References
-
- Jemal A, Bray F, Center MM, Ferlay J, Ward E, Forman D. Global cancer statistics. CA Cancer J Clin. 2011;61:69–90. - PubMed
-
- Chung KY, Gore I, Fong L, Venook A, Beck SB, Dorazio P, et al. Phase II study of the anti-cytotoxic T-lymphocyte-associated antigen 4 monoclonal antibody, tremelimumab, in patients with refractory metastatic colorectal cancer. J Clin Oncol. 2010;28:3485–90. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
