

Urinary kidney biomarkers for early detection of nephrotoxicity in clinical drug development
- PMID: 24219059
- PMCID: PMC4093920
- DOI: 10.1111/bcp.12282
Urinary kidney biomarkers for early detection of nephrotoxicity in clinical drug development
Abstract
Early detection of drug-induced kidney injury is vital in drug development. Generally accepted biomarkers such as creatinine and blood urea nitrogen (BUN) lack sensitivity and early injury responses are missed. Many new biomarkers to detect nephrotoxicity for pre-clinical utilization have been described and their use is adopted in regulatory guidelines. However, guidance on appropriate biomarkers for clinical trials is minimal. We provide an overview of potentially useful kidney biomarkers that can be used in clinical trials. This includes guidance to select biomarkers suitable to capture specific characteristics of the (expected) kidney injury. We conclude that measurement of urinary kidney injury marker-1 (KIM-1) serves many purposes and is often an appropriate choice. Cystatin C captures effects on glomerular filtration rate (GFR), but this marker should preferably be combined with more specific markers to localize the origin of the observed effect. Untoward effects on tubules can be captured relatively well with several markers. Direct detection of glomerular injury is currently impossible since specific biomarkers are lacking. Indirect assessment of toxic effects on glomeruli is possible by using carefully selected panels of other injury markers. We conclude that it is possible to obtain appropriate information on nephrotoxicity in clinical drug development by using carefully selected panels of injury markers and suggest that identification and validation of specific glomerular biomarkers could be of great value.
Keywords: biomarkers; early clinical trials; nephrotoxicity.
© 2013 The British Pharmacological Society.
Figures
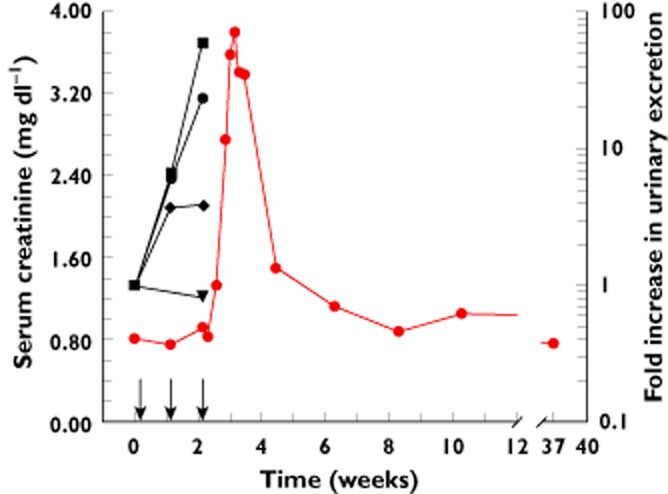
 serum creatinine,
serum creatinine,  urinary B2M,
urinary B2M,  urinary αGST,
urinary αGST,  urinary KIM-1,
urinary KIM-1,  urinary NAG
urinary NAG
References
-
- van Poelgeest EP, Swart RM, Betjes MG, Moerland M, Weening JJ, Tessier Y, Hodges MR, Levin AA, Burggraaf J. Acute kidney injury during therapy with an antisense oligonucleotide directed against PCSK9. Am J Kidney Dis. 2013;62:796–800. - PubMed
-
- Kola I, Landis J. Can the pharmaceutical industry reduce attrition rates. Nat Rev Drug Discov. 2004;3:711–715. - PubMed
-
- Loghman-Adham M, Kiu Weber CI, Ciorciaro C, Mann J, Meier M. Detection and management of nephrotoxicity during drug development. Expert Opin Drug Saf. 2012;11:581–596. - PubMed
-
- McIlroy DR, Wagener G, Lee HT. Biomarkers of acute kidney injury: an evolving domain. Anesthesiology. 2010;112:998–1004. - PubMed
-
- Knight EL, Verhave JC, Spiegelman D, Hillege HL, De ZD, Curhan GC, de Jong PE. Factors influencing serum cystatin C levels other than renal function and the impact on renal function measurement. Kidney Int. 2004;65:1416–1421. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
