

In vivo endomicroscopy improves detection of Barrett's esophagus-related neoplasia: a multicenter international randomized controlled trial (with video)
- PMID: 24219822
- PMCID: PMC4668117
- DOI: 10.1016/j.gie.2013.09.020
In vivo endomicroscopy improves detection of Barrett's esophagus-related neoplasia: a multicenter international randomized controlled trial (with video)
Abstract
Background: Confocal laser endomicroscopy (CLE) enables in vivo microscopic imaging of the GI tract mucosa. However, there are limited data on endoscope-based CLE (eCLE) for imaging Barrett's esophagus (BE).
Objective: To compare high-definition white-light endoscopy (HDWLE) alone with random biopsy (RB) and HDWLE + eCLE and targeted biopsy (TB) for diagnosis of BE neoplasia.
Design: Multicenter, randomized, controlled trial.
Setting: Academic medical centers.
Patients: Adult patients with BE undergoing routine surveillance or referred for early neoplasia.
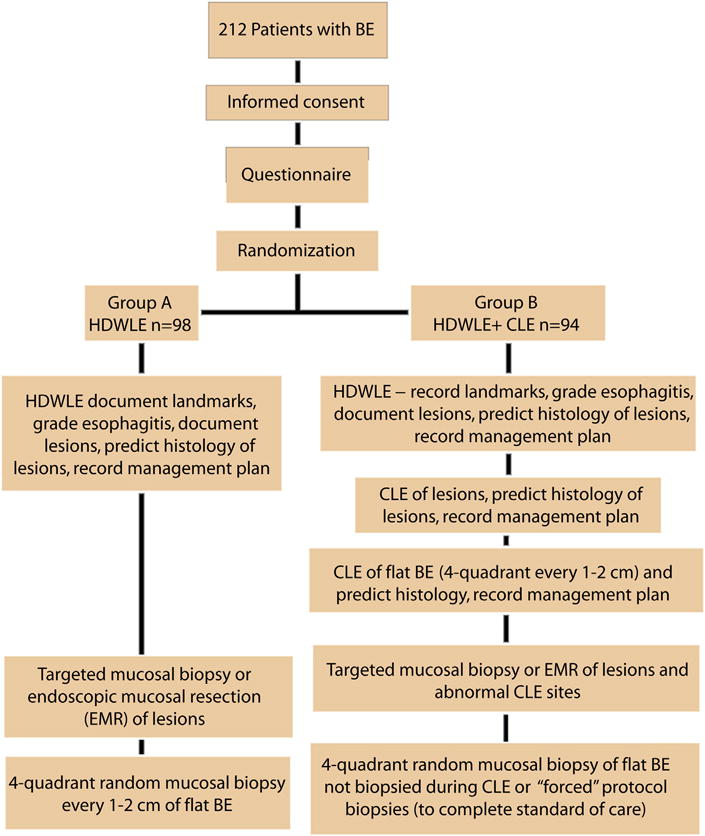
Intervention: Patients were randomized to HDWLE + RB (group 1) or HDWLE + eCLE + TB (group 2). Real-time diagnoses and management plans were recorded after HDWLE in both groups and after eCLE in group 2. Blinded expert pathology diagnosis was the reference standard.
Main outcome measurements: Diagnostic yield, performance characteristics, clinical impact.
Results: A total of 192 patients with BE were studied. HDWLE + eCLE + TB led to a lower number of mucosal biopsies and higher diagnostic yield for neoplasia (34% vs 7%; P < .0001), compared with HDWLE + RB but with comparable accuracy. HDWLE + eCLE + TB tripled the diagnostic yield for neoplasia (22% vs 6%; P = .002) and would have obviated the need for any biopsy in 65% of patients. The addition of eCLE to HDWLE increased the sensitivity for neoplasia detection to 96% from 40% (P < .0001) without significant reduction in specificity. In vivo CLE changed the treatment plan in 36% of patients.
Limitations: Tertiary-care referral centers and expert endoscopists limit generalizability.
Conclusion: Real-time eCLE and TB after HDWLE can improve the diagnostic yield and accuracy for neoplasia and significantly impact in vivo decision making by altering the diagnosis and guiding therapy. (
Clinical trial registration number: NCT01124214.).
Keywords: BE; Barrett's esophagus; CLE; CPT; Current Procedural Terminology; ECA; HDWLE; HGD; NBI; RB; TB; WLE; confocal laser endomicroscopy; eCLE; endoscope-based CLE; esophageal adenocarcinoma; high-definition white-light endoscopy; high-grade dysplasia; narrow-band imaging; pCLE; probe-based CLE; random biopsy; targeted biopsy; white-light endoscopy.
Copyright © 2014 American Society for Gastrointestinal Endoscopy. Published by Mosby, Inc. All rights reserved.
Figures



Comment in
-
Imaging: Advancing dysplasia and neoplasia detection in Barrett oesophagus.Nat Rev Gastroenterol Hepatol. 2014 Jan;11(1):2. doi: 10.1038/nrgastro.2013.229. Epub 2013 Dec 3. Nat Rev Gastroenterol Hepatol. 2014. PMID: 24296577 No abstract available.
-
Surveillance of Barrett's esophagus: why biopsy if you can endomicroscopy.Gastrointest Endosc. 2014 Feb;79(2):222-3. doi: 10.1016/j.gie.2013.11.019. Gastrointest Endosc. 2014. PMID: 24433629 No abstract available.
References
-
- American Gastroenterological A. Spechler SJ, Sharma P, Souza RF, Inadomi JM, Shaheen NJ. American Gastroenterological Association medical position statement on the management of Barrett’s esophagus. Gastroenterology. 2011;140:1084–91. - PubMed
-
- Shaheen NJ, Sharma P, Overholt BF, et al. Radiofrequency ablation in Barrett’s esophagus with dysplasia. N Engl J Med. 2009;360:2277–88. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
