

The impact of body temperature abnormalities on the disease severity and outcome in patients with severe sepsis: an analysis from a multicenter, prospective survey of severe sepsis
- PMID: 24220071
- PMCID: PMC4057086
- DOI: 10.1186/cc13106
The impact of body temperature abnormalities on the disease severity and outcome in patients with severe sepsis: an analysis from a multicenter, prospective survey of severe sepsis
Abstract
Introduction: Abnormal body temperatures (Tb) are frequently seen in patients with severe sepsis. However, the relationship between Tb abnormalities and the severity of disease is not clear. This study investigated the impact of Tb on disease severity and outcomes in patients with severe sepsis.
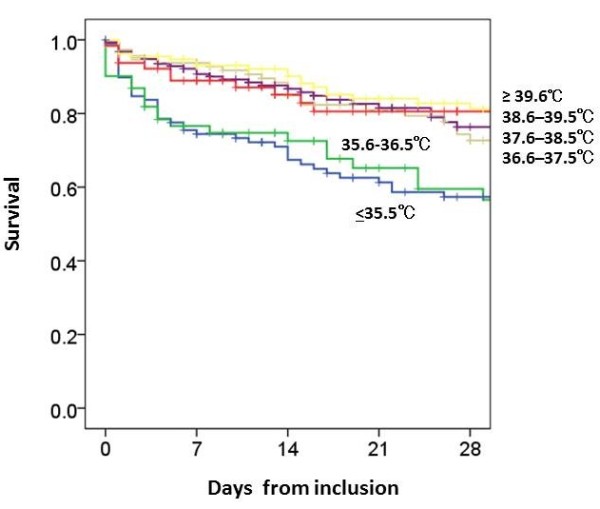
Methods: We enrolled 624 patients with severe sepsis and grouped them into 6 categories according to their Tb at the time of enrollment. The temperature categories (≤ 35.5 °C, 35.6-36.5 °C, 36.6-37.5 °C, 37.6-38.5 °C, 38.6-39.5 °C, ≥ 39.6 °C) were based on the temperature data of the Acute Physiology and Chronic Health Evaluation II (APACHE II) scoring. We compared patient characteristics, physiological data, and mortality between groups.
Results: Patients with Tb of ≤ 36.5 °C had significantly worse sequential organ failure assessment (SOFA) scores when compared with patients with Tb >37.5 °C on the day of enrollment. Scores for APACHE II were also higher in patients with Tb ≤ 35.5 °C when compared with patients with Tb >36.5 °C. The 28-day and hospital mortality was significantly higher in patients with Tb ≤ 36.5 °C. The difference in mortality rate was especially noticeable when patients with Tb ≤ 35.5 °C were compared with patients who had Tb of >36.5 °C. Although mortality did not relate to Tb ranges of ≥ 37.6 °C as compared to reference range of 36.6-37.5 °C, relative risk for 28-day mortality was significantly greater in patients with 35.6-36.5 °C and ≤ 35.5 °C (odds ratio; 2.032, 3.096, respectively). When patients were divided into groups based on the presence (≤ 36.5 °C, n = 160) or absence (>36.5 °C, n = 464) of hypothermia, disseminated intravascular coagulation (DIC) as well as SOFA and APACHE II scores were significantly higher in patients with hypothermia. Patients with hypothermia had significantly higher 28-day and hospital mortality rates than those without hypothermia (38.1% vs. 17.9% and 49.4% vs. 22.6%, respectively). The presence of hypothermia was an independent predictor of 28-day mortality, and the differences between patients with and without hypothermia were observed irrespective of the presence of septic shock.
Conclusions: In patients with severe sepsis, hypothermia (Tb ≤ 36.5 °C) was associated with increased mortality and organ failure, irrespective of the presence of septic shock.
Trial registration: UMIN-CTR ID UMIN000008195.
Figures
Comment in
-
Fever in sepsis: is it cool to be hot?Crit Care. 2014 Feb 13;18(1):109. doi: 10.1186/cc13726. Crit Care. 2014. PMID: 24521542 Free PMC article.
References
-
- O’Grady NP, Barie PS, Bartlett JG, Bleck T, Carroll K, Kalil AC, Linden P, Maki DG, Nierman D, Pasculle W, Masur H. American college of critical care medicine, infectious diseases society of America: guidelines for evaluation of new fever in critically ill adult patients: 2008 update from the American college of critical care medicine and the infectious diseases society of America. Crit Care Med. 2008;17:1330–1349. doi: 10.1097/CCM.0b013e318169eda9. - DOI - PubMed
-
- The Hypothermia after Cardiac Arrest Study Group. Mild therapeutic hypothermia to improve the neurologic outcome after cardiac arrest. N Engl J Med. 2002;17:549–556. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
