

Immunogenicity and safety of a CRM-conjugated meningococcal ACWY vaccine administered concomitantly with routine vaccines starting at 2 months of age
- PMID: 24220326
- PMCID: PMC4185919
- DOI: 10.4161/hv.27051
Immunogenicity and safety of a CRM-conjugated meningococcal ACWY vaccine administered concomitantly with routine vaccines starting at 2 months of age
Abstract
Background: Infants are at the highest risk for meningococcal disease and a broadly protective and safe vaccine is an unmet need in this youngest population. We evaluated the immunogenicity and safety of a 4-dose infant/toddler regimen of MenACWY-CRM given at 2, 4, 6, and 12 months of age concomitantly with pentavalent diphtheria-tetanus-acellular pertussis-Hemophilus influenzae type b-inactivated poliovirus-combination vaccine (DTaP-IPV/Hib), hepatitis B vaccine (HBV), 7- or 13-valent conjugate pneumococcal vaccine (PCV), and measles, mumps, and rubella vaccine (MMR).
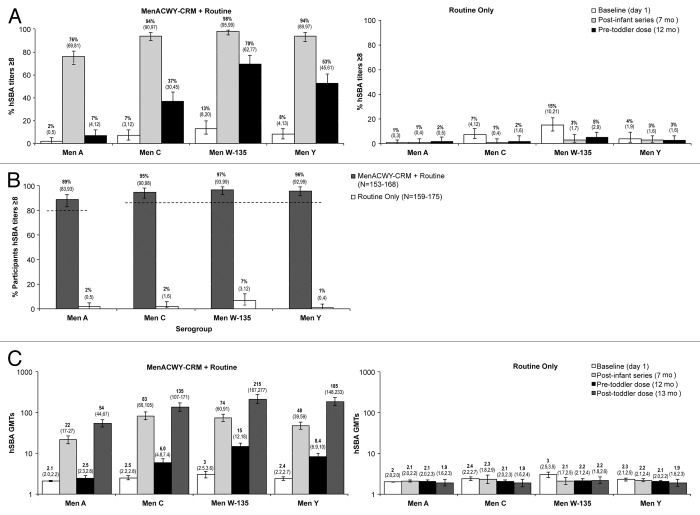
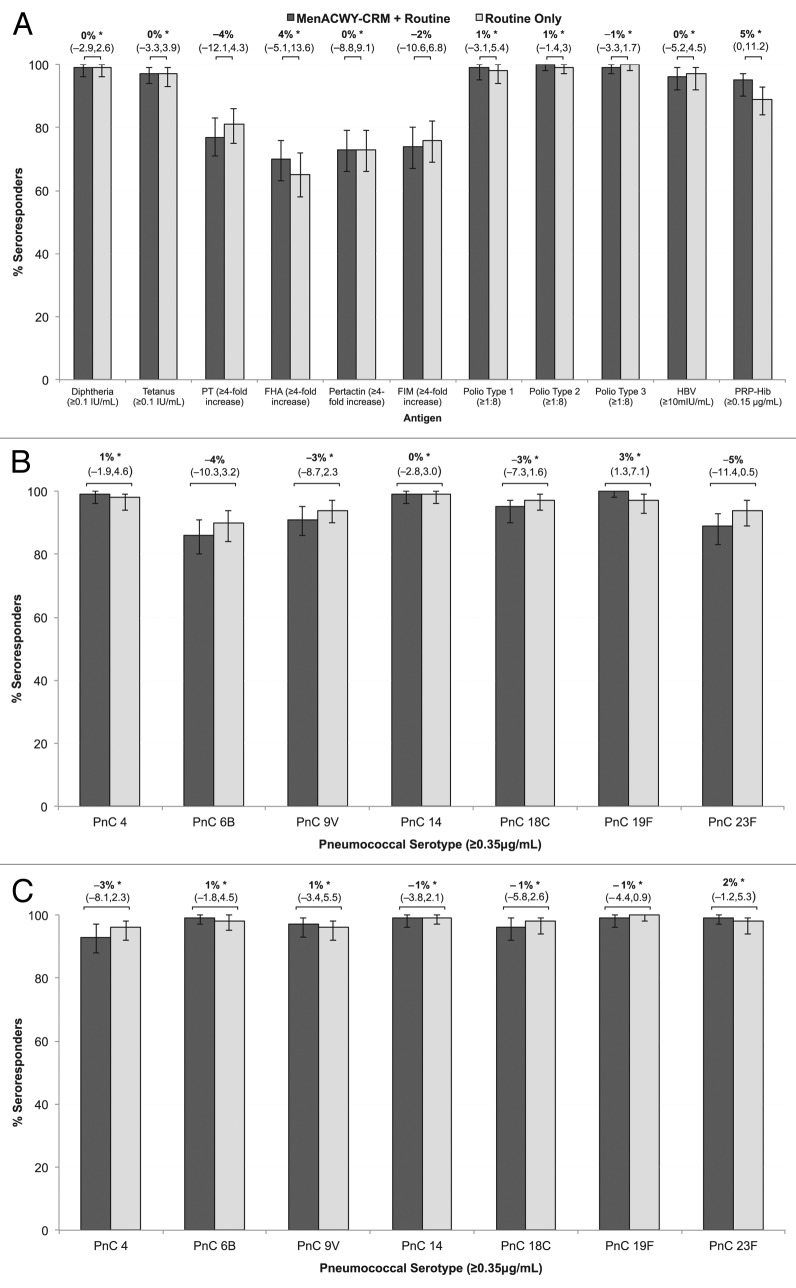
Results: Four doses of MenACWY-CRM induced hSBA titers ≥8 in 89%, 95%, 97%, and 96% of participants against serogroups A, C, W-135, and Y, respectively. hSBA titers ≥8 were present in 76-98% of participants after the first 3 doses. A categorical linear analysis incorporating vaccine group and study center showed responses to routine vaccines administered with MenACWY-CRM were non-inferior to routine vaccines alone, except for seroresponse to the pertussis antigen fimbriae. The reactogenicity profile was not affected when MenACWY-CRM was administered concomitantly with routine vaccines.
Conclusion: MenACWY-CRM administered with routine concomitant vaccinations in young infants was well tolerated and induced highly immunogenic responses against each of the serogroups without significant interference with the immune responses to routine infant vaccinations.
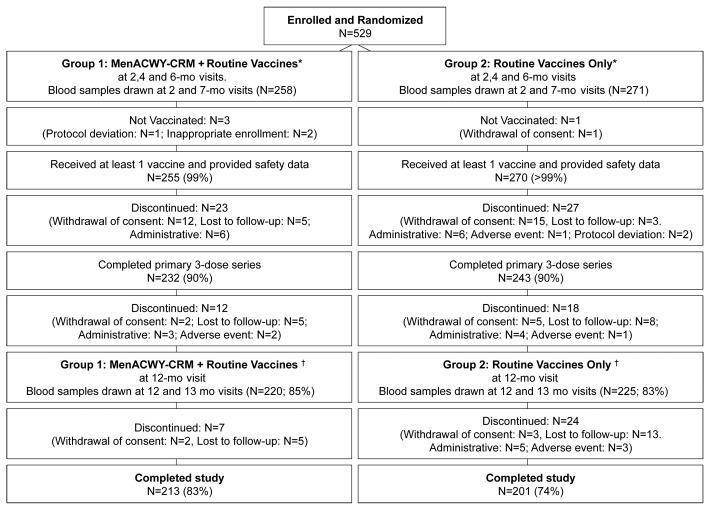
Methods: Healthy 2 month old infants were randomized to receive MenACWY-CRM with routine vaccines (n = 258) or routine vaccines alone (n = 271). Immunogenicity was assessed by serum bactericidal assay using human complement (hSBA). Medically attended adverse events (AEs), serious AEs (SAEs) and AEs leading to study withdrawal were collected throughout the study period.
Keywords: conjugate vaccine; immunogenicity; infants; meningococcal disease; safety.
Figures
References
-
- WHO Meningococcal position paper. Wkly Epidemiol Rec. 2002;44:329–40.
-
- Centers for Disease Control and Prevention. Epidemiology and Prevention of Vaccine-Preventable Diseases. The Pink Book: Course Textbook - 12th Edition (April 2011) http://www.cdc.gov/vaccines/pubs/pinkbook/mening.html Accessed 6 June 2012.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources