

Lipoprotein metabolism, dyslipidemia, and nonalcoholic fatty liver disease
- PMID: 24222095
- PMCID: PMC3988578
- DOI: 10.1055/s-0033-1358519
Lipoprotein metabolism, dyslipidemia, and nonalcoholic fatty liver disease
Abstract
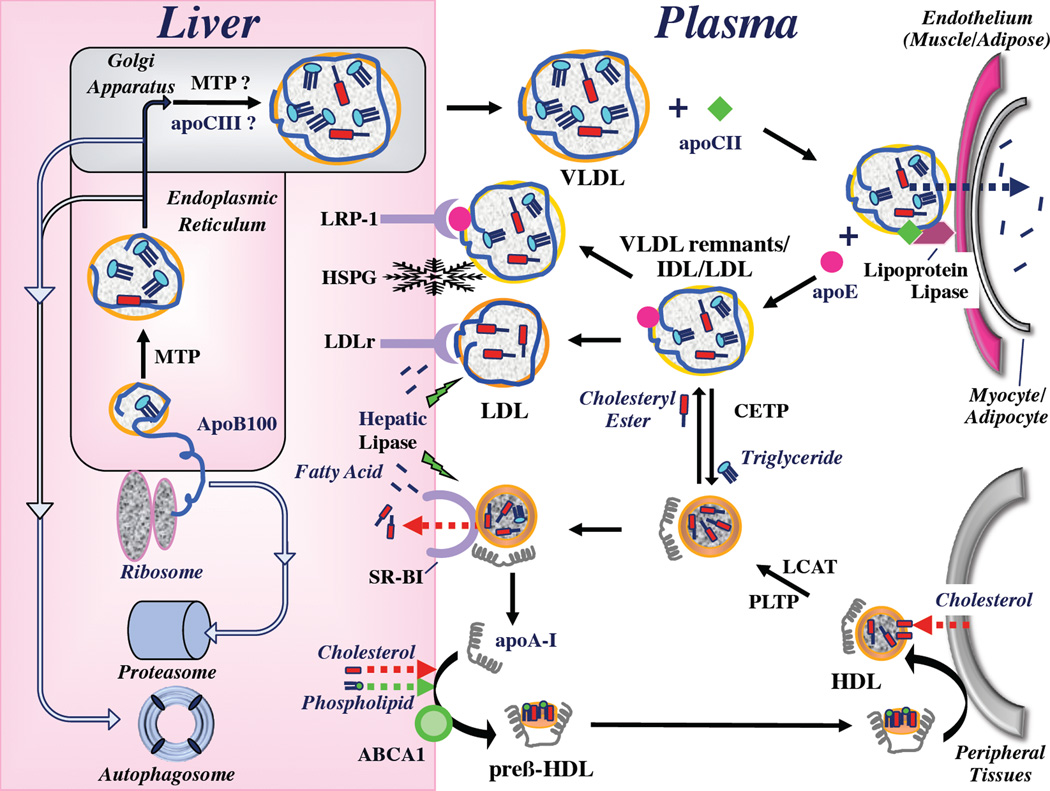
Cardiovascular disease represents the most common cause of death in patients with nonalcoholic fatty liver disease (NAFLD). Patients with NAFLD exhibit an atherogenic dyslipidemia that is characterized by an increased plasma concentration of triglycerides, reduced concentration of high-density lipoprotein (HDL) cholesterol, and low-density lipoprotein (LDL) particles that are smaller and more dense than normal. The pathogenesis of NAFLD-associated atherogenic dyslipidemia is multifaceted, but many aspects are attributable to manifestations of insulin resistance. Here the authors review the structure, function, and metabolism of lipoproteins, which are macromolecular particles of lipids and proteins that transport otherwise insoluble triglyceride and cholesterol molecules within the plasma. They provide a current explanation of the metabolic perturbations that are observed in the setting of insulin resistance. An improved understanding of the pathophysiology of atherogenic dyslipidemia would be expected to guide therapies aimed at reducing morbidity and mortality in patients with NAFLD.
Thieme Medical Publishers 333 Seventh Avenue, New York, NY 10001, USA.
Figures
References
-
- Ekstedt M, Franzen LE, Mathiesen UL, Thorelius L, Holmqvist M, Bodemar G, Kechagias S. Long-term follow-up of patients with NAFLD and elevated liver enzymes. Hepatology. 2006;44:865–873. - PubMed
-
- Vanwagner LB, Bhave M, Te HS, Feinglass J, Alvarez L, Rinella ME. Patients transplanted for nonalcoholic steatohepatitis are at increased risk for postoperative cardiovascular events. Hepatology. 2012;56:1741–1750. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
