

Perinatal outcomes after bariatric surgery: nationwide population based matched cohort study
- PMID: 24222480
- PMCID: PMC3898199
- DOI: 10.1136/bmj.f6460
Perinatal outcomes after bariatric surgery: nationwide population based matched cohort study
Abstract
Objective: To compare perinatal outcomes in births of women with versus without a history of bariatric surgery.
Design: Population based matched cohort study.
Setting: Swedish national health service.
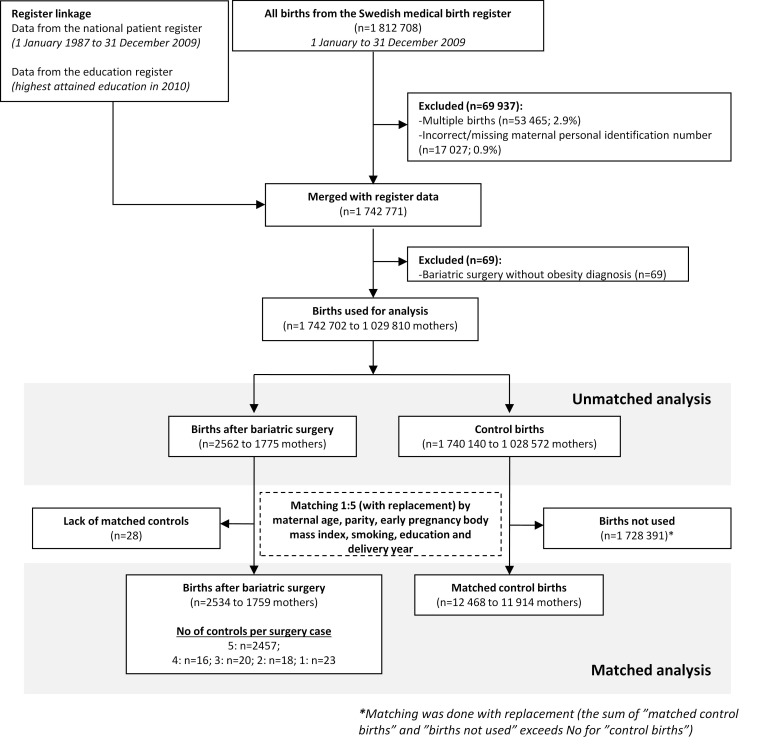
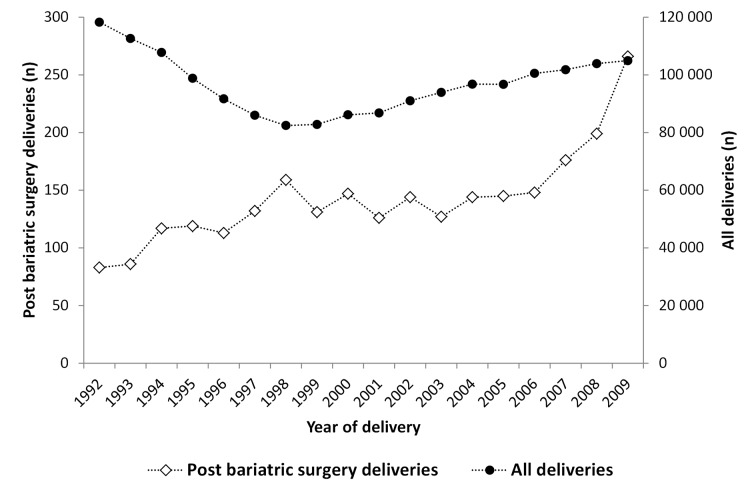
Participants: 1,742,702 singleton births identified in the Swedish medical birth register between 1992 and 2009. For each birth to a mother with a history of bariatric surgery (n=2562), up to five control births were matched by maternal age, parity, early pregnancy body mass index, early pregnancy smoking status, educational level, and year of delivery. Secondary control cohorts, including women eligible for bariatric surgery (body mass index ≥ 35 or ≥ 40), were matched for the same factors except body mass index. History of maternal bariatric surgery was ascertained through the Swedish national patient register from 1980 to 2009.
Main outcome measures: Preterm birth (<37 weeks), small for gestational age birth, large for gestational age birth, stillbirth (≥ 28 weeks), and neonatal death (0-27 days).
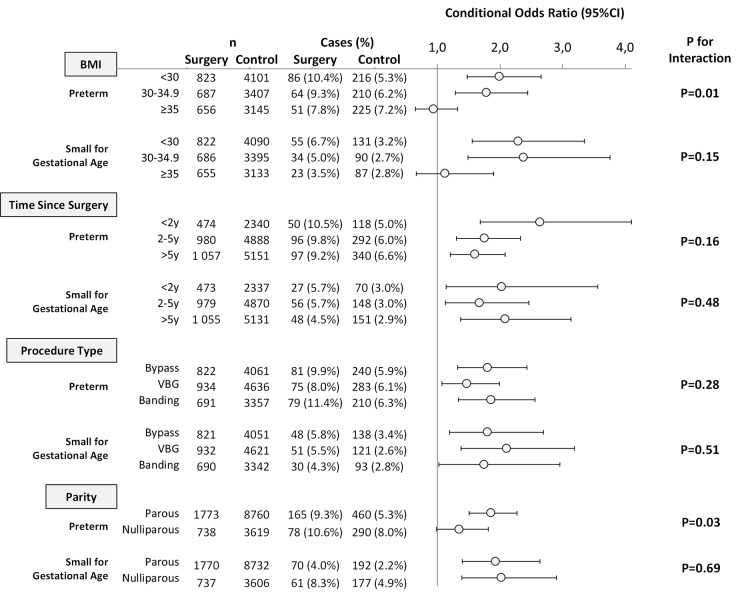
Results: Post-surgery births were more often preterm than in matched controls (9.7% (243/2511) v 6.1% (750/12,379); odds ratio 1.7, 95% confidence interval 1.4 to 2.0; P<0.001). Body mass index seemed to be an effect modifier (P=0.01), and the increased risk of preterm birth was only observed in women with a body mass index <35. A history of bariatric surgery was associated with increased risks of both spontaneous (5.2% (130/2511) v 3.6% (441/12,379); odds ratio 1.5, 1.2 to 1.9; P<0.001) and medically indicated preterm birth (4.5% (113/2511) v 2.5% (309/12,379); odds ratio 1.8, 1.4 to 2.3; P<0.001). A history of bariatric surgery was also associated with an increased risk of a small for gestational age birth (5.2% (131/2507) v 3.0% (369/12,338); odds ratio 2.0, 1.5 to 2.5; P<0.001) and lower risk of a large for gestational age birth (4.2% (105/2507) v 7.3% (895/12,338); odds ratio 0.6, 0.4 to 0.7; P<0.001). No differences were detected for stillbirth or neonatal death. The increased risks for preterm and small for gestational age birth, as well as the decreased risk for large for gestational age birth, remained when post-surgery births were compared with births of women eligible for bariatric surgery.
Conclusion: Women with a history of bariatric surgery were at increased risk of preterm and small for gestational age births and should be regarded as a risk group during pregnancy.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at
Figures
Comment in
-
Women who have had surgery for obesity have raised risk of preterm babies.BMJ. 2013 Nov 12;347:f6774. doi: 10.1136/bmj.f6774. BMJ. 2013. PMID: 24222654 No abstract available.
References
-
- Finucane MM, Stevens GA, Cowan MJ, Danaei G, Lin JK, Paciorek CJ, et al. National, regional, and global trends in body-mass index since 1980: systematic analysis of health examination surveys and epidemiological studies with 960 country-years and 9.1 million participants. Lancet 2011;377:557-67. - PMC - PubMed
-
- Walsh SW. Obesity: a risk factor for preeclampsia. Trends Endocrinol Metab 2007;18:365-70. - PubMed
-
- Singh J, Huang CC, Driggers RW, Timofeev J, Amini D, Landy HJ, et al. The impact of pre-pregnancy body mass index on the risk of gestational diabetes. J Matern Fetal Neonatal Med 2012;25:5-10. - PubMed
-
- Cnattingius S, Bergstrom R, Lipworth L, Kramer MS. Prepregnancy weight and the risk of adverse pregnancy outcomes. N Engl J Med 1998;338:147-52. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical