

Initiation of psychotropic medication after partner bereavement: a matched cohort study
- PMID: 24223722
- PMCID: PMC3818377
- DOI: 10.1371/journal.pone.0077734
Initiation of psychotropic medication after partner bereavement: a matched cohort study
Abstract
Background: Recent changes to diagnostic criteria for depression in DSM-5 remove the bereavement exclusion, allowing earlier diagnosis following bereavement. Evaluation of the potential effect of this change requires an understanding of existing psychotropic medication prescribing by non-specialists after bereavement.
Aims: To describe initiation of psychotropic medication in the first year after partner bereavement.
Methods: In a UK primary care database, we identified 21,122 individuals aged 60 and over with partner bereavement and no psychotropic drug use in the previous year. Prescribing (anxiolytic/hypnotic, antidepressant, antipsychotic) after bereavement was compared to age, sex and practice matched controls.
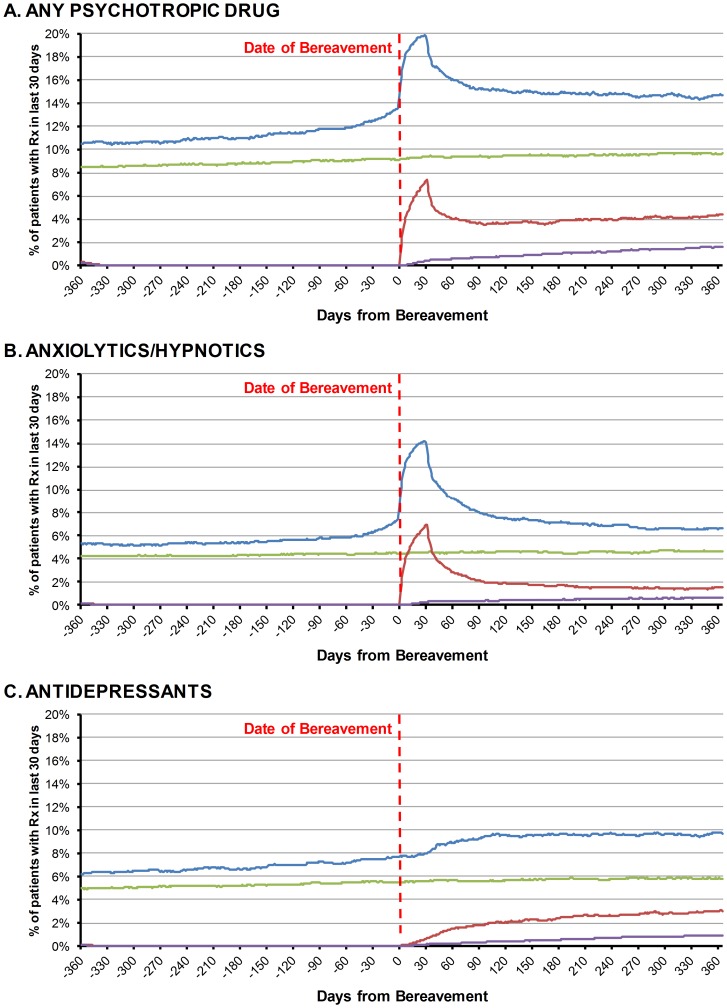
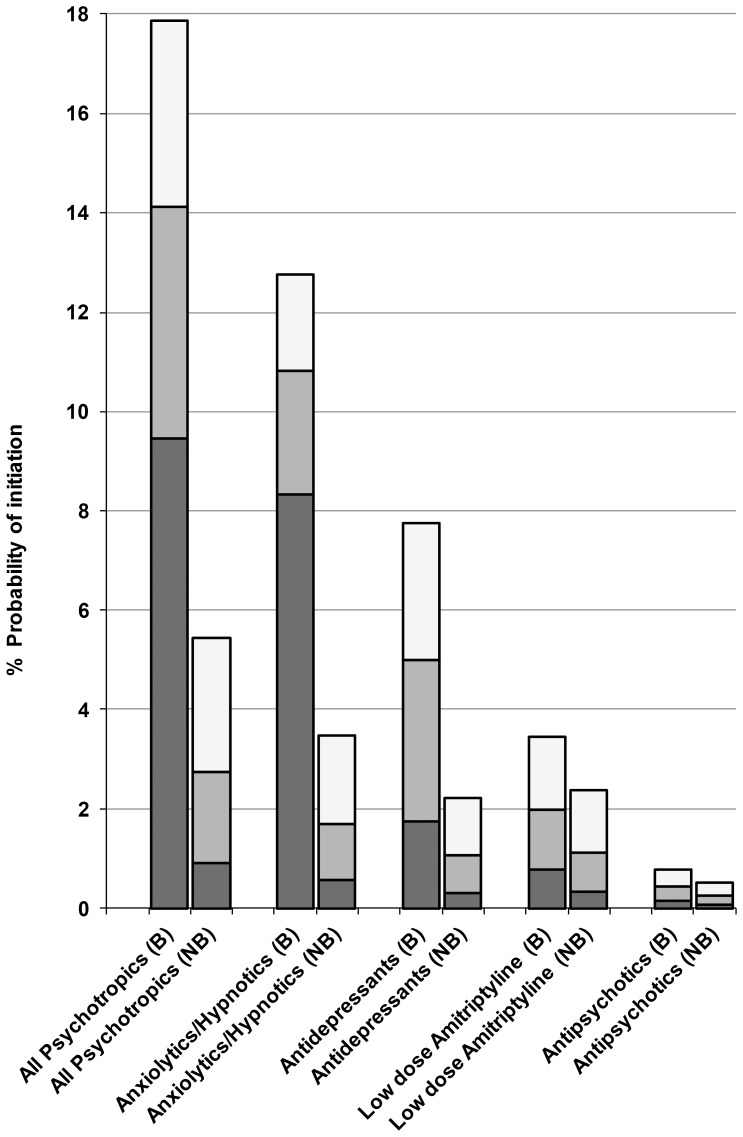
Results: The risks of receiving a new psychotropic prescription within two and twelve months of bereavement were 9.5% (95% CI 9.1 to 9.9%) and 17.9% (17.3 to 18.4%) respectively; an excess risk of initiation in the first year of 12.4% compared to non-bereaved controls. Anxiolytic/hypnotic and antidepressant initiation rates were highest in the first two months. In this period, the hazard ratio for initiation of anxiolytics/hypnotics was 16.7 (95% CI 14.7 to 18.9) and for antidepressants was 5.6 (4.7 to 6.7) compared to non-bereaved controls. 13.3% of those started on anxiolytics/hypnotics within two months continued to receive this drug class at one year. The marked variation in background family practice prescribing of anxiolytics/hypnotics was the strongest determinant of their initiation in the first two months after bereavement.
Conclusion: Almost one in five older people received a new psychotropic drug prescription in the year after bereavement. The early increase and trend in antidepressant use after bereavement suggests some clinicians did not adhere to the bereavement exclusion, with implications for its recent removal in DSM-5. Family practice variation in use of anxiolytics/hypnotics suggests uncertainty over their role in bereavement with the potential for inappropriate long term use.
Conflict of interest statement
Figures
Similar articles
-
Risk for use of antidepressants, anxiolytics, and hypnotics in partners of glioma patients-A nationwide study covering 19 years of prescriptions.Psychooncology. 2018 Aug;27(8):1930-1936. doi: 10.1002/pon.4744. Epub 2018 May 21. Psychooncology. 2018. PMID: 29683227
-
Concomitant psychotropic medication use during treatment of schizophrenia patients: longitudinal results from the CATIE study.Clin Schizophr Relat Psychoses. 2011 Oct;5(3):124-34. doi: 10.3371/CSRP.5.3.2. Clin Schizophr Relat Psychoses. 2011. PMID: 21983496 Clinical Trial.
-
Mortality and medical care after bereavement: a general practice cohort study.PLoS One. 2013;8(1):e52561. doi: 10.1371/journal.pone.0052561. Epub 2013 Jan 25. PLoS One. 2013. PMID: 23372651 Free PMC article.
-
Trends in prescription of psychotropic medications to children and adolescents in Australian primary care from 2011 to 2018.Aust N Z J Psychiatry. 2022 Nov;56(11):1477-1490. doi: 10.1177/00048674211067720. Epub 2021 Dec 28. Aust N Z J Psychiatry. 2022. PMID: 34963342
-
Utilization of antidepressants, anxiolytics, and hypnotics during the COVID-19 pandemic.Transl Psychiatry. 2024 Apr 4;14(1):175. doi: 10.1038/s41398-024-02894-z. Transl Psychiatry. 2024. PMID: 38575574 Free PMC article. Review.
Cited by
-
Grief trajectories and long-term health effects in bereaved relatives: a prospective, population-based cohort study with ten-year follow-up.Front Public Health. 2025 Jul 25;13:1619730. doi: 10.3389/fpubh.2025.1619730. eCollection 2025. Front Public Health. 2025. PMID: 40786154 Free PMC article.
-
New antidepressant utilization pre- and post-bereavement: a population-based study of partners and adult children.Soc Psychiatry Psychiatr Epidemiol. 2020 Oct;55(10):1261-1271. doi: 10.1007/s00127-020-01857-1. Epub 2020 Mar 17. Soc Psychiatry Psychiatr Epidemiol. 2020. PMID: 32185418 Free PMC article.
References
-
- Stroebe M, Schut H, Stroebe W (2007) Health outcomes of bereavement. The Lancet 370(9603): 1960–1973. - PubMed
-
- Editorial (2012) Living with grief. The Lancet 379(9826): 589.
-
- Zisook S, Corruble E, Duan N, Iglewicz A, Karam EG, et al. (2012) The bereavement exclusion and DSM-5. Depress Anxiety 29(5): 425–43. - PubMed
-
- Warner J, Metcalfe C, King M (2001) Evaluating the use of benzodiazepines following recent bereavement. Br J Psychiatry 178(1): 36–41. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
