

The impact of technology diffusion on treatment for prostate cancer
- PMID: 24226306
- PMCID: PMC3916901
- DOI: 10.1097/MLR.0000000000000019
The impact of technology diffusion on treatment for prostate cancer
Abstract
Background: The use of local therapy for prostate cancer may increase because of the perceived advantages of new technologies such as intensity-modulated radiotherapy (IMRT) and robotic prostatectomy.
Objective: To examine the association of market-level technological capacity with receipt of local therapy.
Design: Retrospective cohort.
Subjects: Patients with localized prostate cancer who were diagnosed between 2003 and 2007 (n=59,043) from the Surveillance Epidemiology and End Results-Medicare database.
Measures: We measured the capacity for delivering treatment with new technology as the number of providers offering robotic prostatectomy or IMRT per population in a market (hospital referral region). The association of this measure with receipt of prostatectomy, radiotherapy, or observation was examined with multinomial logistic regression.
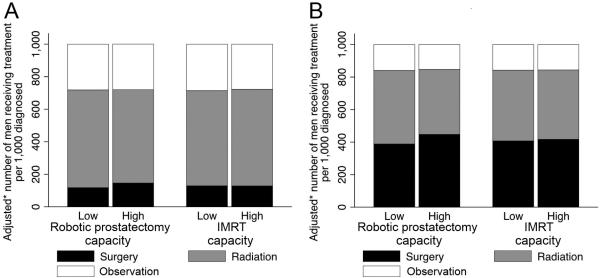
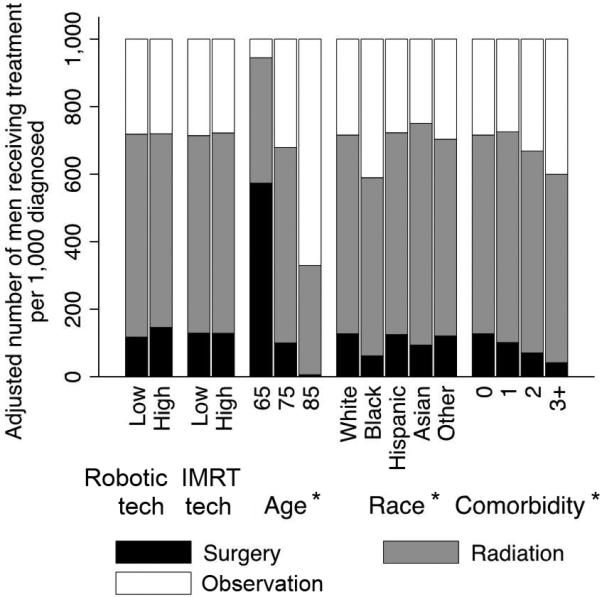
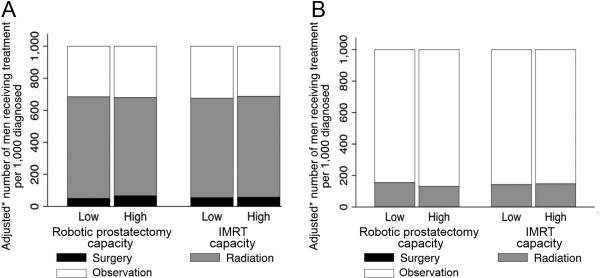
Results: For each 1000 patients diagnosed with prostate cancer, 174 underwent prostatectomy, 490 radiotherapy, and 336 were observed. Markets with high robotic prostatectomy capacity had higher use of prostatectomy (146 vs. 118 per 1000 men, P=0.008) but a trend toward decreased use of radiotherapy (574 vs. 601 per 1000 men, P=0.068), resulting in a stable rate of local therapy. High versus low IMRT capacity did not significantly impact the use of prostatectomy (129 vs. 129 per 1000 men, P=0.947) and radiotherapy (594 vs. 585 per 1000 men, P=0.579).
Conclusions: Although there was a small shift from radiotherapy to prostatectomy in markets with high robotic prostatectomy capacity, increased capacity for both robotic prostatectomy and IMRT did not change the overall rate of local therapy. Our findings temper concerns that the new technology spurs additional therapy of prostate cancer.
Figures
Similar articles
-
Technology diffusion and prostate cancer quality of care.Urology. 2014 Nov;84(5):1066-72. doi: 10.1016/j.urology.2014.06.067. Epub 2014 Oct 24. Urology. 2014. PMID: 25443905 Free PMC article.
-
Technology diffusion and diagnostic testing for prostate cancer.J Urol. 2013 Nov;190(5):1715-20. doi: 10.1016/j.juro.2013.05.007. Epub 2013 May 10. J Urol. 2013. PMID: 23669564 Free PMC article.
-
Use of advanced treatment technologies among men at low risk of dying from prostate cancer.JAMA. 2013 Jun 26;309(24):2587-95. doi: 10.1001/jama.2013.6882. JAMA. 2013. PMID: 23800935 Free PMC article.
-
Cost implications of the rapid adoption of newer technologies for treating prostate cancer.J Clin Oncol. 2011 Apr 20;29(12):1517-24. doi: 10.1200/JCO.2010.31.1217. Epub 2011 Mar 14. J Clin Oncol. 2011. PMID: 21402604 Free PMC article.
-
Management of localised prostate cancer: watchful waiting, surgery or radiation therapy, depending on the natural course, which is often relatively slow.Prescrire Int. 2012 Oct;21(131):242-8. Prescrire Int. 2012. PMID: 23185849 Review.
Cited by
-
Technology diffusion and prostate cancer quality of care.Urology. 2014 Nov;84(5):1066-72. doi: 10.1016/j.urology.2014.06.067. Epub 2014 Oct 24. Urology. 2014. PMID: 25443905 Free PMC article.
-
Variation in the use of postoperative radiotherapy among high-risk patients following radical prostatectomy.Prostate Cancer Prostatic Dis. 2016 Jun;19(2):216-21. doi: 10.1038/pcan.2016.9. Epub 2016 Mar 8. Prostate Cancer Prostatic Dis. 2016. PMID: 26951715
-
The Effect of the Diffusion of the Surgical Robot on the Hospital-level Utilization of Partial Nephrectomy.Med Care. 2015 Jan;53(1):71-8. doi: 10.1097/MLR.0000000000000259. Med Care. 2015. PMID: 25494234 Free PMC article.
-
Creating a National Provider Identifier (NPI) to Unique Physician Identification Number (UPIN) Crosswalk for Medicare Data.Med Care. 2017 Dec;55(12):e113-e119. doi: 10.1097/MLR.0000000000000462. Med Care. 2017. PMID: 29135774 Free PMC article.
-
What Promotes Surgeon Practice Change? A Scoping Review of Innovation Adoption in Surgical Practice.Ann Surg. 2021 Mar 1;273(3):474-482. doi: 10.1097/SLA.0000000000004355. Ann Surg. 2021. PMID: 33055590 Free PMC article.
References
-
- Newhouse JP. Medical care costs: how much welfare loss? J Econ Perspect. 1992;6:3–21. - PubMed
-
- Maxwell S, Zuckerman S, Berenson RA. Use of Physicians’ Services under Medicare's Resource-Based Payments. N. Engl. J. Med. 2007;356:1853–1861. - PubMed
-
- Medicare Payment Advisory Commission [March 12, 2013];March 2012 Report to the Congress: Medicare Payment Policy. 2012 Available at: http://medpac.gov/documents/Mar12_EntireReport.pdf.
-
- Cutler DM, McClellan M. Is technological change in medicine worth it? Health Affairs. 2001;20:11–29. - PubMed
-
- Legorreta AP, Silber JH, Costantino GN, et al. Increased cholecystectomy rate after the introduction of laparoscopic cholecystectomy. JAMA. 1993;270:1429–1432. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
