

SGLT2 inhibitor empagliflozin reduces renal growth and albuminuria in proportion to hyperglycemia and prevents glomerular hyperfiltration in diabetic Akita mice
- PMID: 24226524
- PMCID: PMC3920018
- DOI: 10.1152/ajprenal.00520.2013
SGLT2 inhibitor empagliflozin reduces renal growth and albuminuria in proportion to hyperglycemia and prevents glomerular hyperfiltration in diabetic Akita mice
Abstract
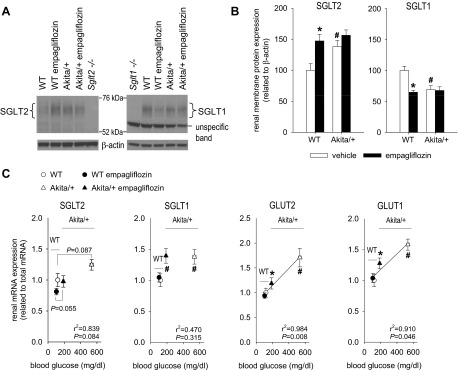
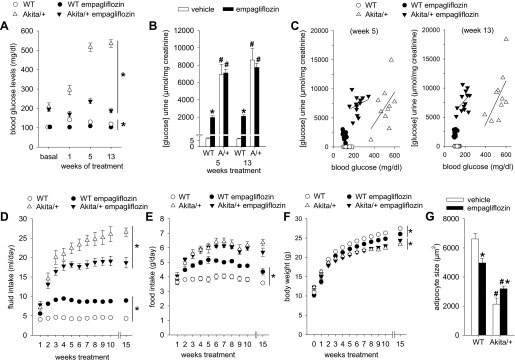
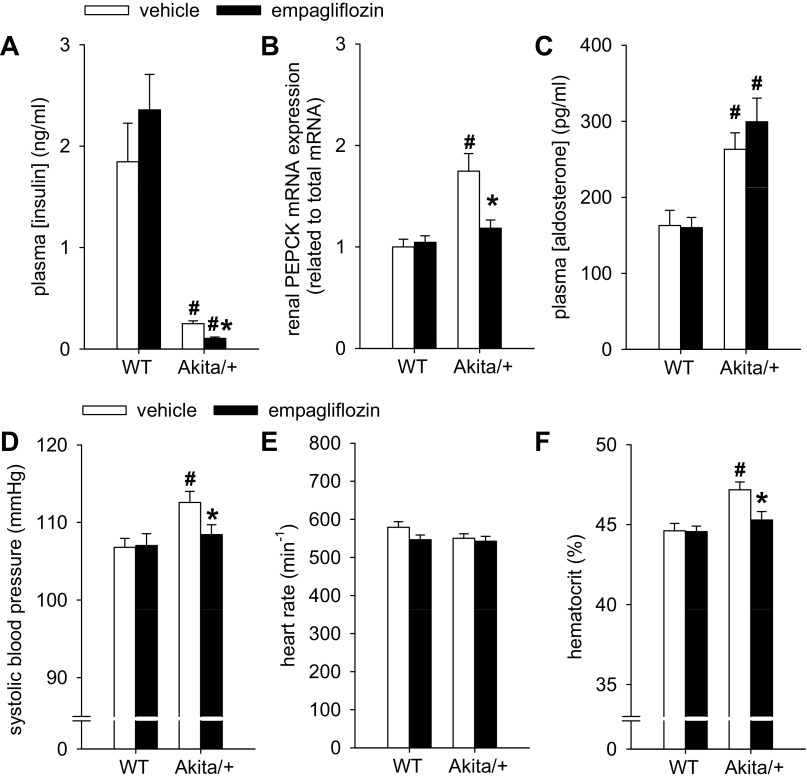
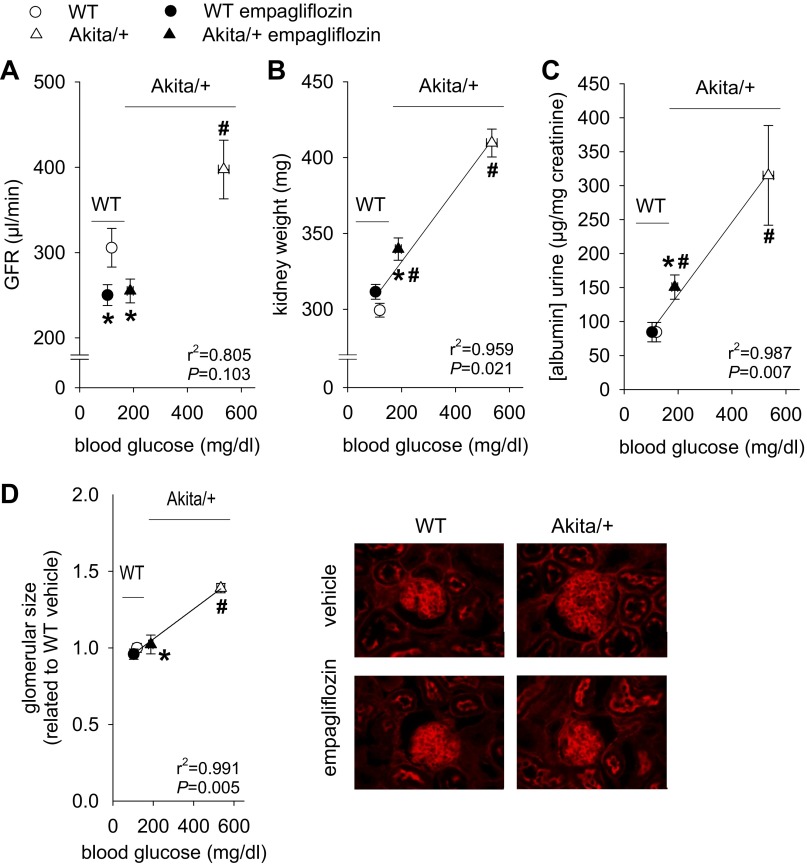
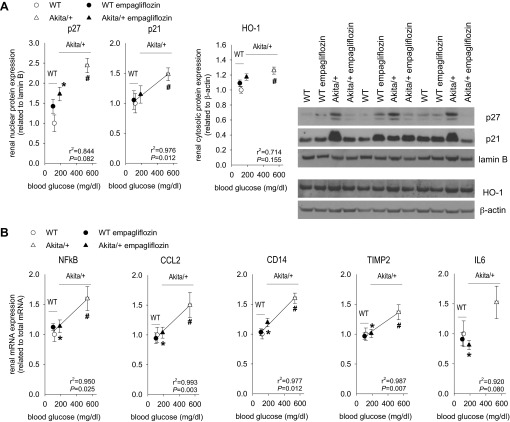
Our previous work has shown that gene knockout of the sodium-glucose cotransporter SGLT2 modestly lowered blood glucose in streptozotocin-diabetic mice (BG; from 470 to 300 mg/dl) and prevented glomerular hyperfiltration but did not attenuate albuminuria or renal growth and inflammation. Here we determined effects of the SGLT2 inhibitor empagliflozin (300 mg/kg of diet for 15 wk; corresponding to 60-80 mg·kg(-1)·day(-1)) in type 1 diabetic Akita mice that, opposite to streptozotocin-diabetes, upregulate renal SGLT2 expression. Akita diabetes, empagliflozin, and Akita + empagliflozin similarly increased renal membrane SGLT2 expression (by 38-56%) and reduced the expression of SGLT1 (by 33-37%) vs. vehicle-treated wild-type controls (WT). The diabetes-induced changes in SGLT2/SGLT1 protein expression are expected to enhance the BG-lowering potential of SGLT2 inhibition, and empagliflozin strongly lowered BG in Akita (means of 187-237 vs. 517-535 mg/dl in vehicle group; 100-140 mg/dl in WT). Empagliflozin modestly reduced GFR in WT (250 vs. 306 μl/min) and completely prevented the diabetes-induced increase in glomerular filtration rate (GFR) (255 vs. 397 μl/min). Empagliflozin attenuated increases in kidney weight and urinary albumin/creatinine ratio in Akita in proportion to hyperglycemia. Empagliflozin did not increase urinary glucose/creatinine ratios in Akita, indicating the reduction in filtered glucose balanced the inhibition of glucose reabsorption. Empagliflozin attenuated/prevented the increase in systolic blood pressure, glomerular size, and molecular markers of kidney growth, inflammation, and gluconeogenesis in Akita. We propose that SGLT2 inhibition can lower GFR independent of reducing BG (consistent with the tubular hypothesis of diabetic glomerular hyperfiltration), while attenuation of albuminuria, kidney growth, and inflammation in the early diabetic kidney may mostly be secondary to lower BG.
Keywords: diabetes; diabetic nephropathy; gluconeogenesis; inflammation; phosphoenolpyruvate carboxykinase; proximal tubule; renal growth.
Figures
References
-
- Balen D, Ljubojevic M, Breljak D, Brzica H, Zlender V, Koepsell H, Sabolic I. Revised immunolocalization of the Na+-d-glucose cotransporter SGLT1 in rat organs with an improved antibody. Am J Physiol Cell Physiol 295: C475–C489, 2008 - PubMed
-
- Baumgartl HJ, Sigl G, Banholzer P, Haslbeck M, Standl E. On the prognosis of IDDM patients with large kidneys. Nephrol Dial Transplant 13: 630–634, 1998 - PubMed
-
- Bognetti E, Zoja A, Meschi F, Paesano PL, Chiumello G. Relationship between kidney volume, microalbuminuria and duration of diabetes mellitus. Diabetologia 39: 1409, 1996 - PubMed
-
- Cherney DZ, Perkins BA, Soleymanlou N, Maione M, Lai V, Lee A, Fagan NM, Woerle HJ, Johansen OE, Broedl UC, von Eynatten M. Renal hemodynamic effect of sodium-glucose cotransporter 2 inhibition in patients with type 1 diabetes mellitus. Circulation. [E pub before print] - PubMed
-
- Christiansen JS, Gammelgaard J, Frandsen M, Parving HH. Increased kidney size, glomerular filtration rate and renal plasma flow in short-term insulin-dependent diabetics. Diabetologia 20: 451–456, 1981 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases