

Association between insomnia symptoms and mortality: a prospective study of U.S. men
- PMID: 24226807
- PMCID: PMC3987964
- DOI: 10.1161/CIRCULATIONAHA.113.004500
Association between insomnia symptoms and mortality: a prospective study of U.S. men
Abstract
Background: Insomnia complaints are common in older adults and may be associated with mortality risk. However, evidence regarding this association is mixed. Thus, we prospectively examined whether men with insomnia symptoms had an increased risk of mortality during 6 years of follow-up.
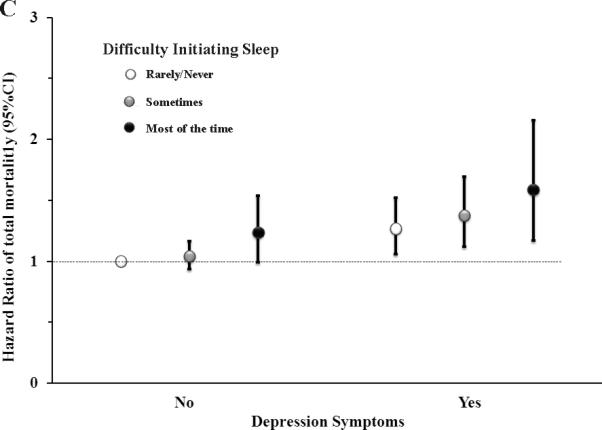
Methods and results: A prospective cohort study of 23,447 US men participating in the Health Professionals Follow-Up Study and free of cancer, reported on insomnia symptoms in 2004, were followed through 2010. Deaths were identified from state vital statistic records, the National Death Index, family reports, and the postal system. We documented 2025 deaths during 6 years of follow-up (2004-2010). The multivariable-adjusted hazard ratios of total mortality were 1.25 (95% confidence interval [CI], 1.04-1.50) for difficulty initiating sleep, 1.09 (95% CI, 0.97-1.24) for difficulty maintaining sleep, 1.04 (95% CI, 0.88-1.22) for early-morning awakenings, and 1.24 (95% CI, 1.05-1.46) for nonrestorative sleep, comparing men with those symptoms most of the time with men without those symptoms, after adjusting for age, lifestyle factors, and presence of common chronic conditions. Men with difficulty initiating sleep and nonrestorative sleep most of the time had a 55% (hazard ratio, 1.55; 95% CI, 1.19-2.04; P-trend=0.01) and 32% (hazard ratio, 1.32; 95% CI, 1.02-1.72; P-trend=0.002) increased risk of cardiovascular disease mortality, respectively, relative to men without those symptoms.
Conclusion: Some insomnia symptoms, especially difficulty initiating asleep and nonrestorative sleep, are associated with a modestly higher risk of mortality.
Keywords: cardiovascular disease; meta-analysis; mortality; sleep disorders; sleep initiation and maintenance disorders.
Figures




References
-
- National Institute of Health [October 19, 2012];Insomnia. http://www.nhlbi.nih.gov/health/public/sleep/insomnia.pdf.
-
- Edinger JD, Bonnet MH, Bootzin RR, Doghramji K, Dorsey CM, Espie CA, Jamieson AO, McCall WV, Morin CM, Stepanski EJ, American Academy of Sleep Medicine Work Group Derivation of research diagnostic criteria for insomnia: report of an American Academy of Sleep Medicine Work Group. Sleep. 2004;27:1567–1596. - PubMed
-
- Carskadon MA, Brown ED, Dement WC. Sleep fragmentation in the elderly: relationship to daytime sleep tendency. Neurobiol Aging. 1982;3:321–327. - PubMed
-
- Carskadon MA, van den Hoed J, Dement WC. Sleep and daytime sleepiness in the elderly. J Geriatr Psychiatry. 1980;13:135–151. - PubMed
-
- Prinz PN, Vitiello MV, Raskind MA, Thorpy MJ. Geriatrics: Sleep disorders and aging. N Engl J Med. 1990;323:520–526. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
