

Portal vein embolization improves rate of resection of extensive colorectal liver metastases without worsening survival
- PMID: 24227364
- PMCID: PMC5527845
- DOI: 10.1002/bjs.9317
Portal vein embolization improves rate of resection of extensive colorectal liver metastases without worsening survival
Abstract
Background: Most patients requiring an extended right hepatectomy (ERH) have an inadequate standardized future liver remnant (sFLR) and need preoperative portal vein embolization (PVE). However, the clinical and oncological impact of PVE in such patients remains unclear.
Methods: All consecutive patients presenting at the M. D. Anderson Cancer Center with colorectal liver metastases (CLM) requiring ERH at presentation from 1995 to 2012 were studied. Surgical and oncological outcomes were compared between patients with adequate and inadequate sFLRs at presentation.
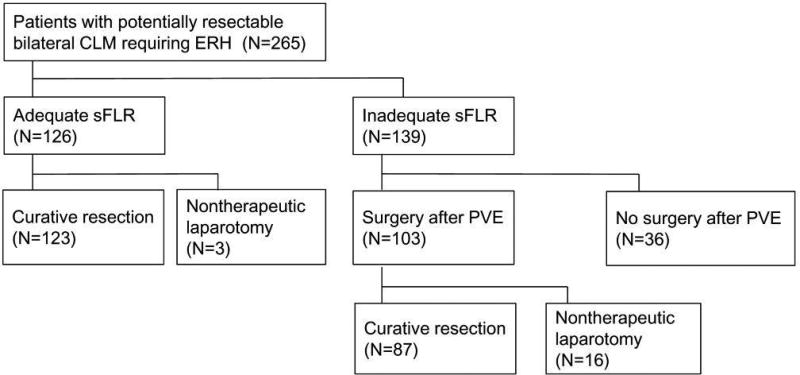
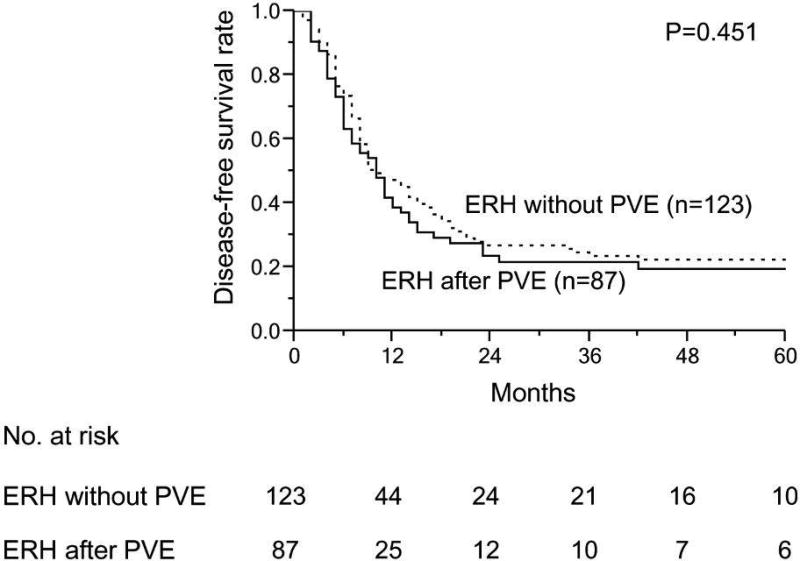
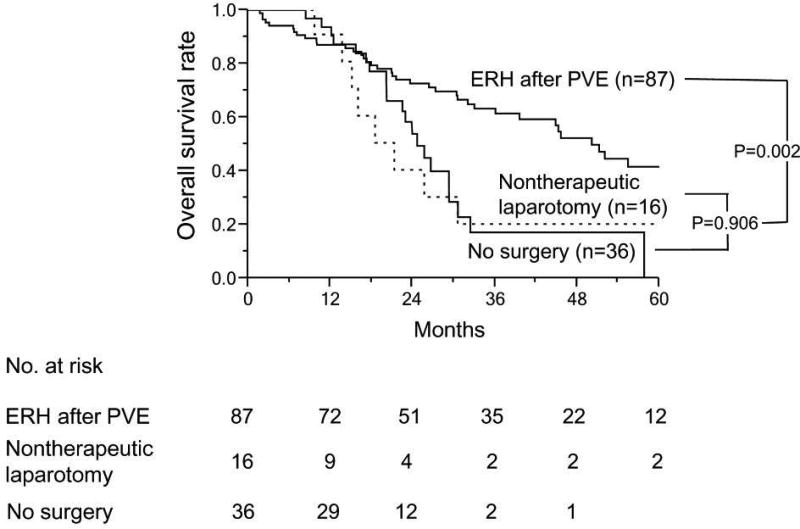
Results: Of the 265 patients requiring ERH, 126 (47·5 per cent) had an adequate sFLR at presentation, of whom 123 underwent a curative resection. Of the 139 patients (52·5 per cent) who had an inadequate sFLR and underwent PVE, 87 (62·6 per cent) had a curative resection. Thus, the curative resection rate was increased from 46·4 per cent (123 of 265) at baseline to 79·2 per cent (210 of 265) following PVE. Among patients who underwent ERH, major complication and 90-day mortality rates were similar in the no-PVE and PVE groups (22·0 and 4·1 per cent versus 31 and 7 per cent respectively); overall and disease-free survival rates were also similar in these two groups. Of patients with an inadequate sFLR at presentation, those who underwent ERH had a significantly better median overall survival (50·2 months) than patients who had non-curative surgery (21·3 months) or did not undergo surgery (24·7 months) (P = 0·002).
Conclusion: PVE enabled curative resection in two-thirds of patients with CLM who had an inadequate sFLR and were unable to tolerate ERH at presentation. Patients who underwent curative resection after PVE had overall and disease-free survival rates equivalent to those of patients who did not need PVE.
© 2013 British Journal of Surgery Society Ltd. Published by John Wiley & Sons Ltd.
Figures

References
-
- Elias D, Ouellet JF, De Baere T, Lasser P, Roche A. Preoperative selective portal vein embolization before hepatectomy for liver metastases: long-term results and impact on survival. Surgery. 2002;131:294–299. - PubMed
-
- Kishi Y, Abdalla EK, Chun YS, Zorzi D, Madoff DC, Wallace MJ, et al. Three hundred and one consecutive extended right hepatectomies: evaluation of outcome based on systematic liver volumetry. Ann Surg. 2009;250:540–548. - PubMed
-
- Kubota K, Makuuchi M, Kusaka K, Kobayashi T, Miki K, Hasegawa K, et al. Measurement of liver volume and hepatic functional reserve as a guide to decision-making in resectional surgery for hepatic tumors. Hepatology. 1997;26:1176–1181. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
