

Opioid utilization and opioid-related adverse events in nonsurgical patients in US hospitals
- PMID: 24227700
- PMCID: PMC3976956
- DOI: 10.1002/jhm.2102
Opioid utilization and opioid-related adverse events in nonsurgical patients in US hospitals
Abstract
Background: Recent studies in the outpatient setting have demonstrated high rates of opioid prescribing and overdose-related deaths. Prescribing practices in hospitalized patients are unexamined.
Objective: To investigate patterns and predictors of opioid utilization in nonsurgical admissions to US hospitals, variation in use, and the association between hospital-level use and rates of severe opioid-related adverse events.
Design, setting, and patients: Adult nonsurgical admissions to 286 US hospitals.
Measurements: Opioid exposure and severe opioid-related adverse events during hospitalization, defined using hospital charges and International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) codes.
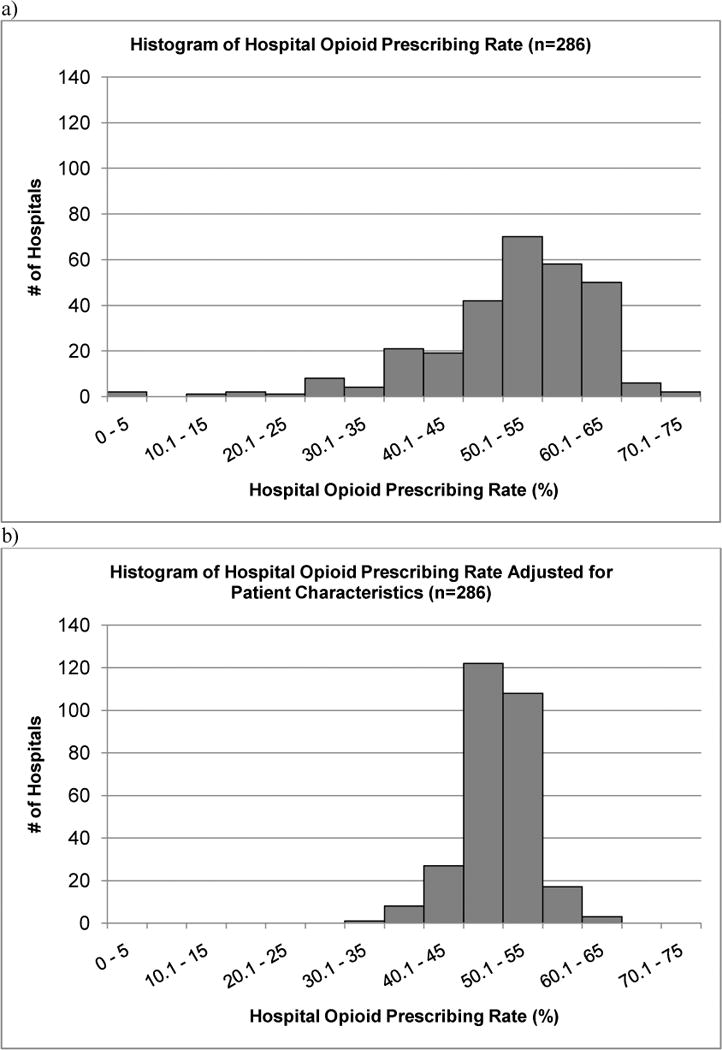
Results: Of 1.14 million admissions, opioids were used in 51%. The mean ± standard deviation daily dose received in oral morphine equivalents was 68 ± 185 mg; 23% of exposed received a total daily dose of ≥100 mg oral morphine equivalents. Opioid-prescribing rates ranged from 5% in the lowest-prescribing hospital to 72% in the highest-prescribing hospital (mean, 51% ± 10%). After adjusting for patient characteristics, the adjusted opioid-prescribing rates ranged from 33% to 64% (mean, 50% ± standard deviation 4%). Among exposed, 0.60% experienced severe opioid-related adverse events. Hospitals with higher opioid-prescribing rates had higher adjusted relative risk of a severe opioid-related adverse event per patient exposed (relative risk: 1.23 [1.14-1.33] for highest-prescribing compared with lowest-prescribing quartile).
Conclusions: The majority of hospitalized nonsurgical patients were exposed to opioids, often at high doses. Hospitals that used opioids most frequently had increased adjusted risk of a severe opioid-related adverse event per patient exposed. Interventions to standardize and enhance the safety of opioid prescribing in hospitalized patients should be investigated.
© 2013 Society of Hospital Medicine.
Conflict of interest statement
Figures
References
-
- Okie S. A flood of opioids, a rising tide of deaths. N Engl J Med. 2010;363(21):1981–5. - PubMed
-
- Paulozzi LJ, Budnitz DS, Xi Y. Increasing deaths from opioid analgesics in the United States. Pharmacoepidemiol Drug Saf. 2006;15(9):618–27. - PubMed
-
- Pletcher MJ, Kertesz SG, Kohn MA, Gonzales R. Trends in opioid prescribing by race/ethnicity for patients seeking care in US emergency departments. JAMA. 2008;299(1):70–8. - PubMed
-
- Joranson DE, Ryan KM, Gilson AM, Dahl JL. Trends in medical use and abuse of opioid analgesics. JAMA. 2000;283(13):1710–4. - PubMed
-
- Bohnert AS, Valenstein M, Bair MJ, Ganoczy D, McCarthy JF, Ilgen MA, et al. Association between opioid prescribing patterns and opioid overdose-related deaths. JAMA. 2011;305(13):1315–21. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
