

Phase 3 study of recombinant factor VIII Fc fusion protein in severe hemophilia A
- PMID: 24227821
- PMCID: PMC3894491
- DOI: 10.1182/blood-2013-10-529974
Phase 3 study of recombinant factor VIII Fc fusion protein in severe hemophilia A
Abstract
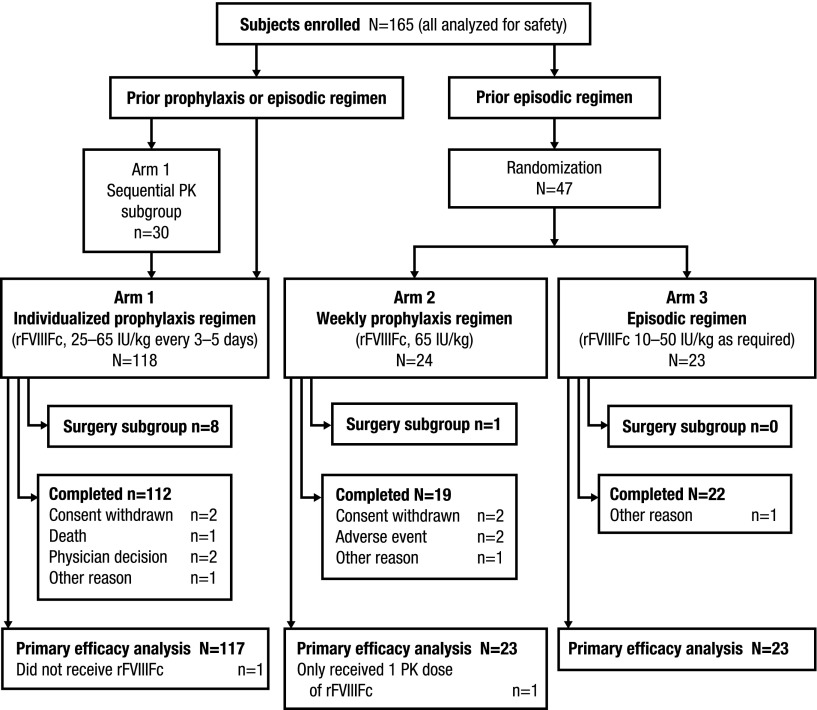
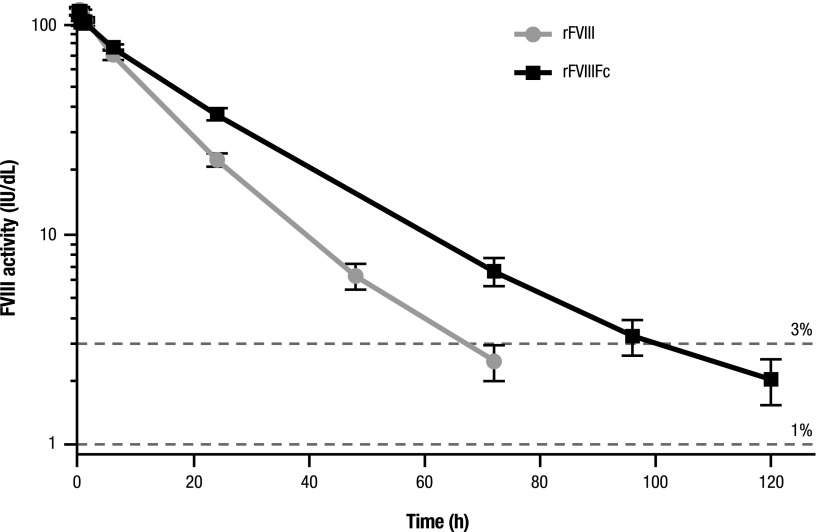
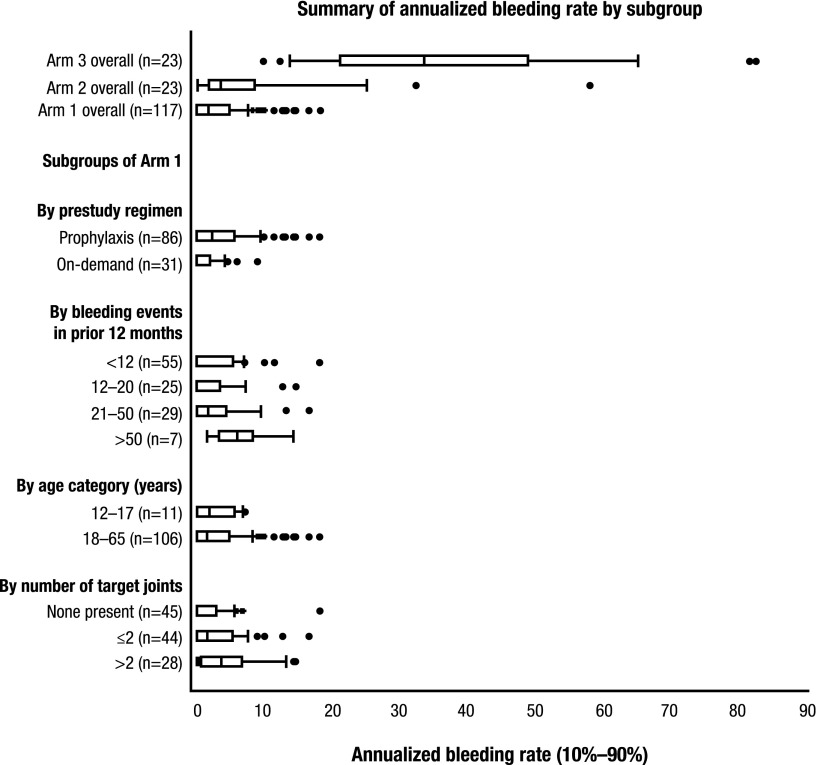
This phase 3 pivotal study evaluated the safety, efficacy, and pharmacokinetics of a recombinant FVIII Fc fusion protein (rFVIIIFc) for prophylaxis, treatment of acute bleeding, and perioperative hemostatic control in 165 previously treated males aged ≥12 years with severe hemophilia A. The study had 3 treatment arms: arm 1, individualized prophylaxis (25-65 IU/kg every 3-5 days, n = 118); arm 2, weekly prophylaxis (65 IU/kg, n = 24); and arm 3, episodic treatment (10-50 IU/kg, n = 23). A subgroup compared recombinant FVIII (rFVIII) and rFVIIIFc pharmacokinetics. End points included annualized bleeding rate (ABR), inhibitor development, and adverse events. The terminal half-life of rFVIIIFc (19.0 hours) was extended 1.5-fold vs rFVIII (12.4 hours; P < .001). Median ABRs observed in arms 1, 2, and 3 were 1.6, 3.6, and 33.6, respectively. In arm 1, the median weekly dose was 77.9 IU/kg; approximately 30% of subjects achieved a 5-day dosing interval (last 3 months on study). Across arms, 87.3% of bleeding episodes resolved with 1 injection. Adverse events were consistent with those expected in this population; no subjects developed inhibitors. rFVIIIFc was well-tolerated, had a prolonged half-life compared with rFVIII, and resulted in low ABRs when dosed prophylactically 1 to 2 times per week.
Trial registration: ClinicalTrials.gov NCT01181128.
Figures
Comment in
-
A longer acting rFVIII, safe and effective.Blood. 2014 Jan 16;123(3):304-5. doi: 10.1182/blood-2013-12-539825. Blood. 2014. PMID: 24434992
References
-
- Fogarty PF. Biological rationale for new drugs in the bleeding disorders pipeline. Hematology Am Soc Hematol Educ Program 2011;2011:397-404. - PubMed
-
- National Hemophilia Foundation. MASAC recommendation concerning prophylaxis (regular administration of clotting factor concentrate to prevent bleeding). Available at: http://www.hemophilia.org/NHFWeb/MainPgs/MainNHF.aspx?menuid=57&contenti.... Accessed July 18, 2013.
-
- Lillicrap D. Improvements in factor concentrates. Curr Opin Hematol. 2010;17(5):393–397. - PubMed
-
- Hacker MR, Geraghty S, Manco-Johnson M. Barriers to compliance with prophylaxis therapy in haemophilia. Haemophilia. 2001;7(4):392–396. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
