

Antidepressant augmentation using the N-methyl-D-aspartate antagonist memantine: a randomized, double-blind, placebo-controlled trial
- PMID: 24229746
- PMCID: PMC4000742
- DOI: 10.4088/JCP.12m08252
Antidepressant augmentation using the N-methyl-D-aspartate antagonist memantine: a randomized, double-blind, placebo-controlled trial
Abstract
Objective: Intravenous N-methyl-d-aspartate (NMDA) antagonists have shown promising results in rapidly ameliorating depression symptoms, but placebo-controlled trials of oral NMDA antagonists as monotherapy have not observed efficacy. We conducted a randomized, double-blind, placebo-controlled trial of the NMDA antagonist memantine as an augmentation treatment for patients with DSM-IV major depressive disorder.
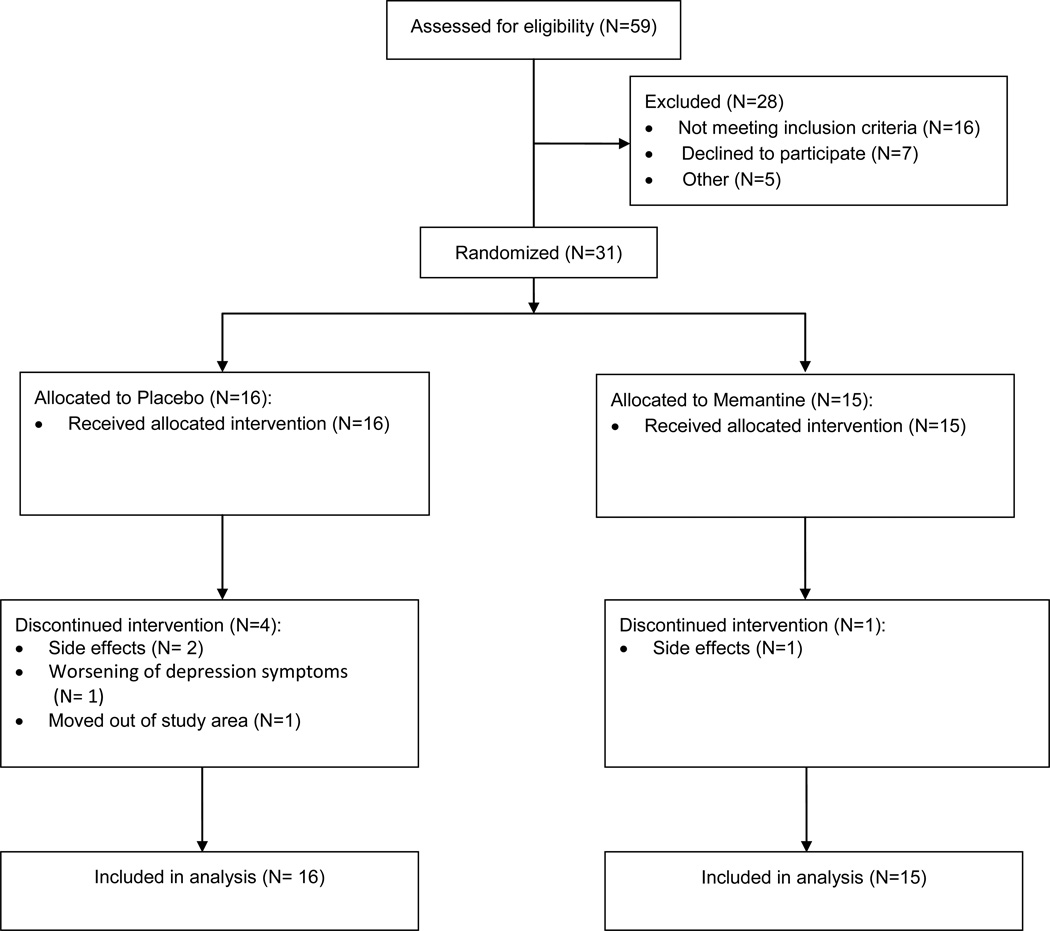
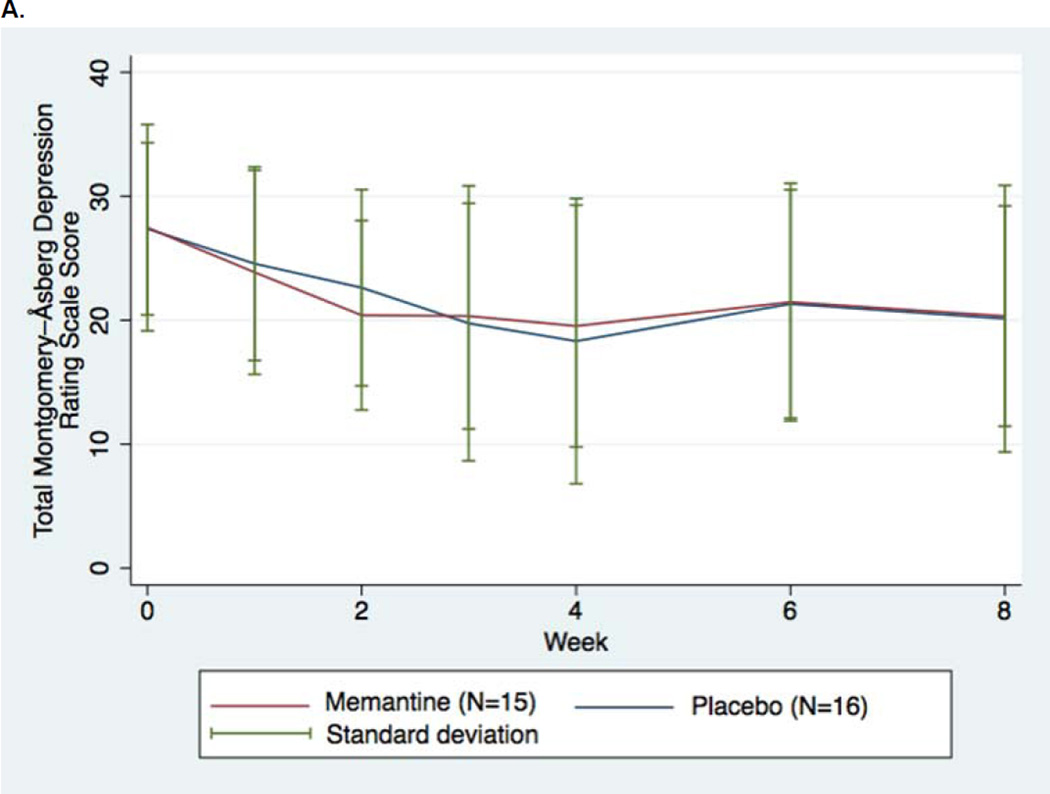
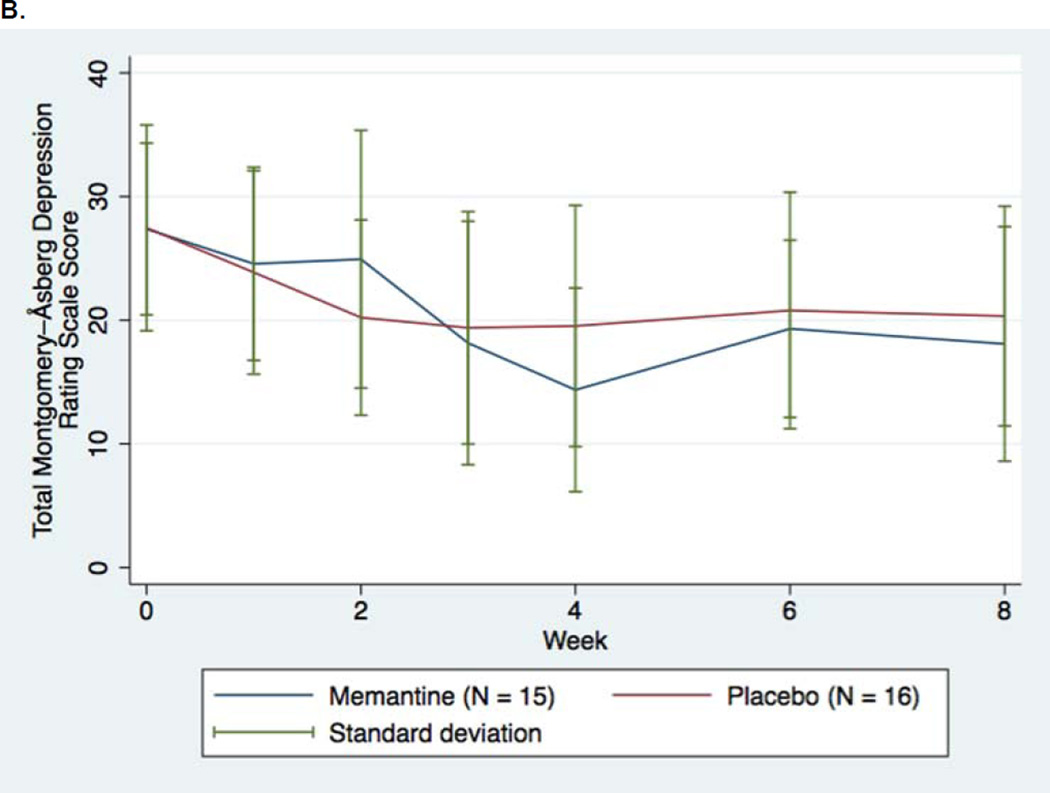
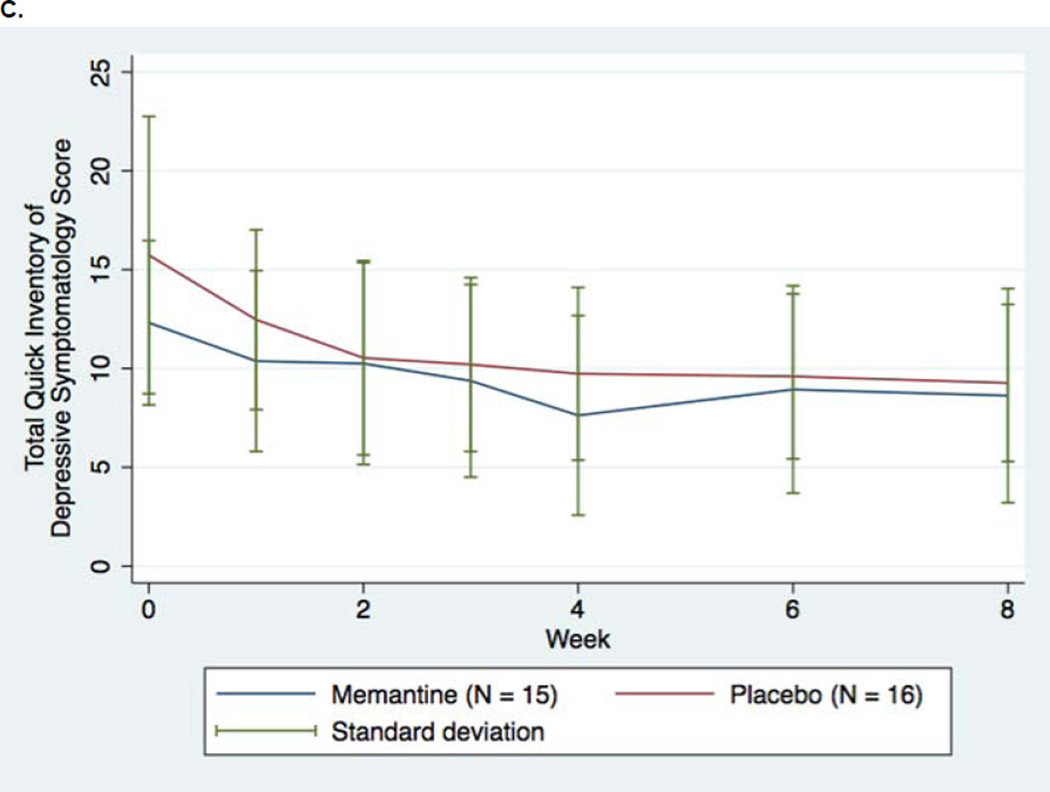
Method: Adult outpatients with major depressive disorder and partial response or nonresponse to their current antidepressant (as indicated by a 17-item Hamilton Depression Rating Scale score of ≥ 16 at baseline) were randomized (from July 2006-December 2011) to add memantine (flexible dose 5-20 mg/d, with all memantine group participants reaching the dose of 20 mg/d) (n = 15) or placebo (n = 16) to their existing treatment for 8 weeks. The primary outcome, change in Montgomery-Asberg Depression Rating Score (MADRS), was evaluated with repeated-measures mixed effects models using last-observation-carried-forward methods. Secondary outcomes included other depression and anxiety rating scales, suicidal and delusional ideation, and other adverse effects.
Results: 84% of participants completed the trial, including 93% of participants receiving memantine. Participants receiving memantine did not show a statistically or clinically significant change in MADRS scores compared to placebo, either over the entire study (β = 0.133, favoring placebo, P = .74) or at study completion (week 8 mean [SD] MADRS score change = -7.13 [6.61] [memantine]; -7.25 [11.14] [placebo]; P = .97). A minimal to small effect size (comparing change to baseline variability) favoring placebo was observed (Cohen d = 0.19). Similarly, no substantial effect sizes favoring memantine nor statistically significant between-group differences were observed on secondary efficacy outcomes.
Conclusions: This trial did not detect significant statistical or effect size differences between memantine and placebo augmentation among nonresponders or poor responders to conventional antidepressants. While the small number of participants is a limitation, this study suggests memantine lacks substantial efficacy as an augmentation treatment for major depressive disorder.
Trial registration: ClinicalTrials.gov identifier: NCT00344682.
© Copyright 2013 Physicians Postgraduate Press, Inc.
Figures
References
-
- Zarate CA, Jr, Singh JB, Carlson PJ, et al. A randomized trial of an N-methyl-D-aspartate antagonist in treatment-resistant major depression. Arch Gen Psychiatry. 2006;63(8):856–864. - PubMed
-
- Berman RM, Cappiello A, Anand A, et al. Antidepressant effects of ketamine in depressed patients. Biol Psychiatry. 2000;47(4):351–354. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
