

Human Treg responses allow sustained recombinant adeno-associated virus-mediated transgene expression
- PMID: 24231351
- PMCID: PMC3859421
- DOI: 10.1172/JCI70314
Human Treg responses allow sustained recombinant adeno-associated virus-mediated transgene expression
Abstract
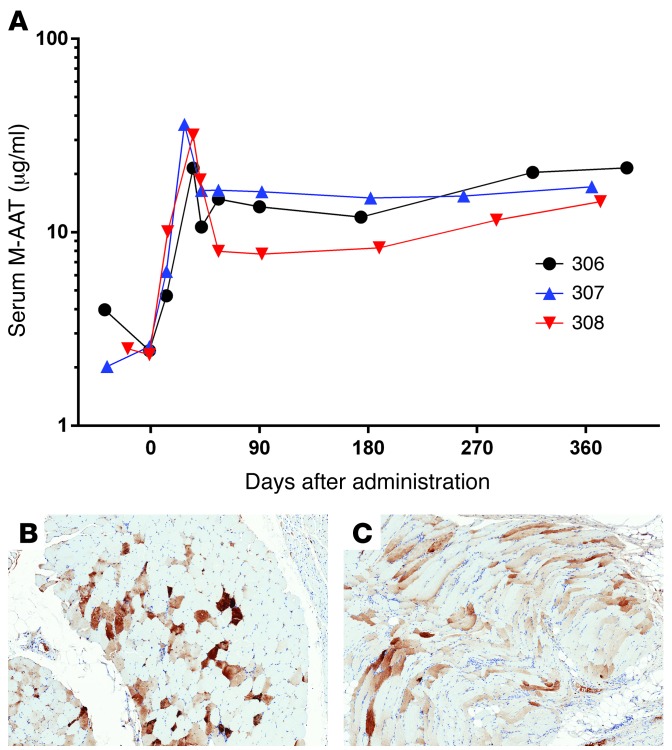
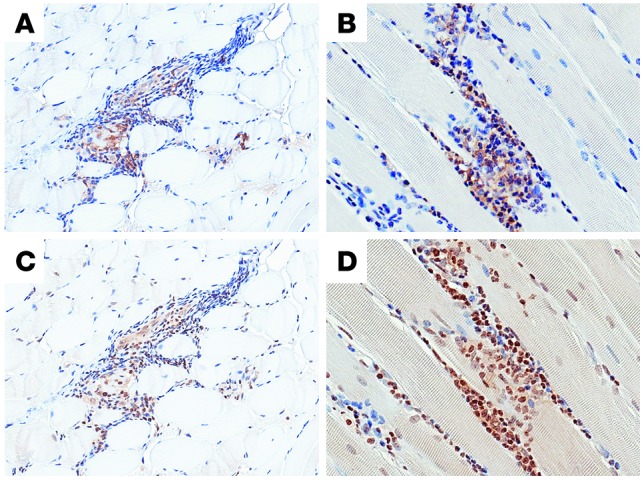
Recombinant adeno-associated virus (rAAV) vectors have shown promise for the treatment of several diseases; however, immune-mediated elimination of transduced cells has been suggested to limit and account for a loss of efficacy. To determine whether rAAV vector expression can persist long term, we administered rAAV vectors expressing normal, M-type α-1 antitrypsin (M-AAT) to AAT-deficient subjects at various doses by multiple i.m. injections. M-specific AAT expression was observed in all subjects in a dose-dependent manner and was sustained for more than 1 year in the absence of immune suppression. Muscle biopsies at 1 year had sustained AAT expression and a reduction of inflammatory cells compared with 3 month biopsies. Deep sequencing of the TCR Vβ region from muscle biopsies demonstrated a limited number of T cell clones that emerged at 3 months after vector administration and persisted for 1 year. In situ immunophenotyping revealed a substantial Treg population in muscle biopsy samples containing AAT-expressing myofibers. Approximately 10% of all T cells in muscle were natural Tregs, which were activated in response to AAV capsid. These results suggest that i.m. delivery of rAAV type 1-AAT (rAAV1-AAT) induces a T regulatory response that allows ongoing transgene expression and indicates that immunomodulatory treatments may not be necessary for rAAV-mediated gene therapy.
Figures





References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
