

Indications for valve-pressure adjustments of gravitational assisted valves in patients with idiopathic normal pressure hydrocephalus
- PMID: 24231878
- PMCID: PMC3814988
- DOI: 10.4103/2152-7806.119879
Indications for valve-pressure adjustments of gravitational assisted valves in patients with idiopathic normal pressure hydrocephalus
Abstract
Background: Modern ventriculoperitoneal shunts (VPS) are programmable, which enables clinicians to adjust valve-pressure according to their patients' individual needs. The aim of this retrospective analysis is to evaluate indications for valve-pressure adjustments in idiopathic normal pressure hydrocephalus (iNPH).
Methods: Patients operated between 2004 and 2011 diagnosed with iNPH were included. Kiefer-Scale was used to classify each patient. Follow-up exams were conducted 3, 6, and 12 months after shunt implantation and yearly thereafter. Initial valve-pressure was 100 or 70 mmH2O. Planned reductions of the valve-pressure to 70 and 50 mmH2O, respectively, were carried out and reactive adjustment of the valve-pressure to avoid over- and under-drainage were indicated.
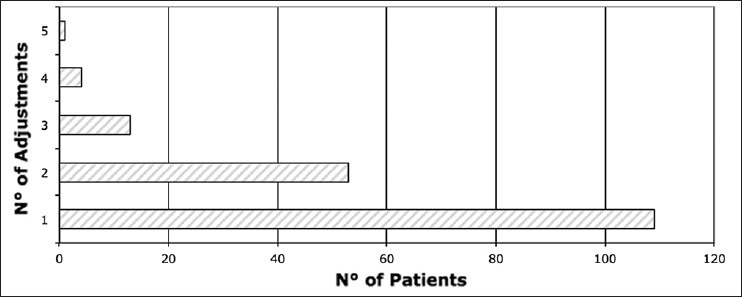
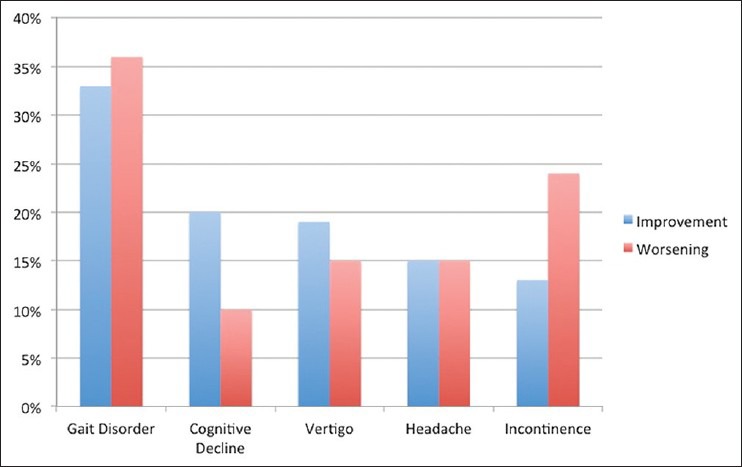
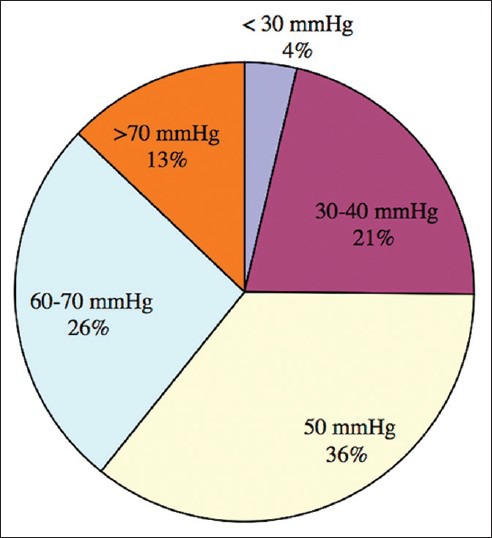
Results: A total of 52 patients were provided with a Medos-Hakim valve(Codman®) with a Miethke shunt-assistant(Aesculap®) and 111 patients with a Miethke-proGAV(Aesculap®). 180 reductions of the valve-pressure took place (65% reactive, 35% planned). Most patients (89%) needed one or two adjustments of their valve-pressures for optimal results. In 41%, an improvement of the symptoms was observed. Gait disorder was improved most often after valve-pressure adjustments (32%). 18 times an elevation of valve-pressure was necessary because of headaches, vertigo, or the development of subdural hygroma. Optimal valve-pressure for most patients was around 50 mmH2O (36%).
Conclusion: The goal of shunt therapy in iNPH should usually be valve-pressure settings between 30 and 70 mmH2O. Reactive adjustments of the valve-pressure are useful for therapy of over- and underdrainage symptoms. Planned reductions of the valve opening pressure are effective even if postoperative results are already satisfactory.
Keywords: Adjustments; gravitational valve; iNPH; idiopathic normal pressure hydrocephalus; indications; valve-pressure.
Figures
Similar articles
-
Patients benefit from low-pressure settings enabled by gravitational valves in normal pressure hydrocephalus.Clin Neurol Neurosurg. 2013 Oct;115(10):1982-6. doi: 10.1016/j.clineuro.2013.06.010. Epub 2013 Jul 4. Clin Neurol Neurosurg. 2013. PMID: 23831048
-
Improved outcome in shunted iNPH with a combination of a Codman Hakim programmable valve and an Aesculap-Miethke ShuntAssistant.Cent Eur Neurosurg. 2010 Aug;71(3):113-6. doi: 10.1055/s-0029-1241179. Epub 2010 Apr 6. Cent Eur Neurosurg. 2010. PMID: 20373276
-
An investigation into the clinical impacts of lowering shunt opening pressure in idiopathic normal pressure hydrocephalus: A case series.Br J Neurosurg. 2015 Feb;29(1):18-22. doi: 10.3109/02688697.2014.950630. Epub 2014 Aug 21. Br J Neurosurg. 2015. PMID: 25142701
-
The programmable shunt-system Codman Medos Hakim: A clinical observation study and review of literature.Clin Neurol Neurosurg. 2018 Oct;173:154-158. doi: 10.1016/j.clineuro.2018.08.023. Epub 2018 Aug 13. Clin Neurol Neurosurg. 2018. PMID: 30142621 Review.
-
Reconsidering Ventriculoperitoneal Shunt Surgery and Postoperative Shunt Valve Pressure Adjustment: Our Approaches Learned From Past Challenges and Failures.Front Neurol. 2022 Jan 6;12:798488. doi: 10.3389/fneur.2021.798488. eCollection 2021. Front Neurol. 2022. PMID: 35069426 Free PMC article. Review.
Cited by
-
Single center experiences with telemetric intracranial pressure measurements in patients with CSF circulation disturbances.Acta Neurochir (Wien). 2020 Oct;162(10):2487-2497. doi: 10.1007/s00701-020-04421-7. Epub 2020 Jun 3. Acta Neurochir (Wien). 2020. PMID: 32495080 Free PMC article.
-
Ventriculoperitoneal shunt malfunction due to chronic cholecystitis: A case report.Medicine (Baltimore). 2020 Jun 19;99(25):e20565. doi: 10.1097/MD.0000000000020565. Medicine (Baltimore). 2020. PMID: 32569180 Free PMC article.
-
Optimization of number and range of shunt valve performance levels in infant hydrocephalus: a machine learning analysis.Front Bioeng Biotechnol. 2024 Mar 18;12:1352490. doi: 10.3389/fbioe.2024.1352490. eCollection 2024. Front Bioeng Biotechnol. 2024. PMID: 38562668 Free PMC article.
-
Programmable gravitational valves in idiopathic normal pressure hydrocephalus: long-term outcomes after a 3-year follow-up.Acta Neurochir (Wien). 2025 May 24;167(1):151. doi: 10.1007/s00701-025-06563-y. Acta Neurochir (Wien). 2025. PMID: 40411615 Free PMC article.
-
5-Year health-related quality of life outcome in patients with idiopathic normal pressure hydrocephalus.J Neurol. 2021 Sep;268(9):3283-3293. doi: 10.1007/s00415-021-10477-x. Epub 2021 Mar 2. J Neurol. 2021. PMID: 33651154 Free PMC article.
References
-
- Akiguchi I, Ishii M, Watanabe Y, Watanabe T, Kawasaki T, Yagi H, et al. Shunt-responsive parkinsonism and reversible white matter lesions in patients with idiopathic NPH. J Neurol. 2008;255:1392–9. - PubMed
-
- Hashimoto MA. Development of shunt technology especially for idiopathic normal pressure hydrocephalus. Brain Nerve. 2008;60:247–55. - PubMed
-
- Kiefer M, Eymann R, Komenda Y, Steudel WI. Ein Graduierungssystem für den chronischen Hydrozephalus. A Grading System for Chronic Hydrocephalus. Zentralbl Neurochir. 2003;64:109–15. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
