

Radiological diagnosis and management of epistaxis
- PMID: 24232035
- PMCID: PMC3895177
- DOI: 10.1007/s00270-013-0776-y
Radiological diagnosis and management of epistaxis
Abstract
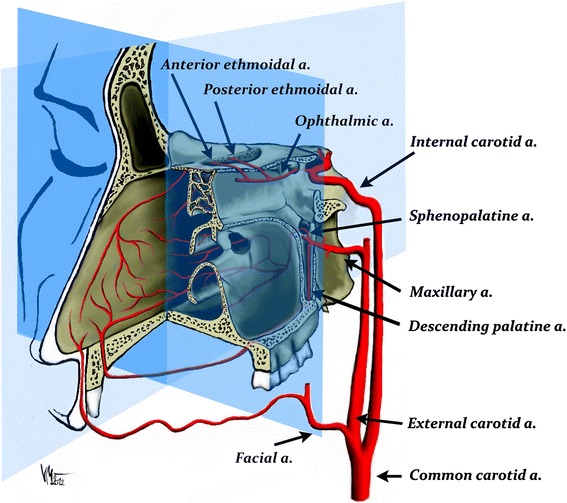
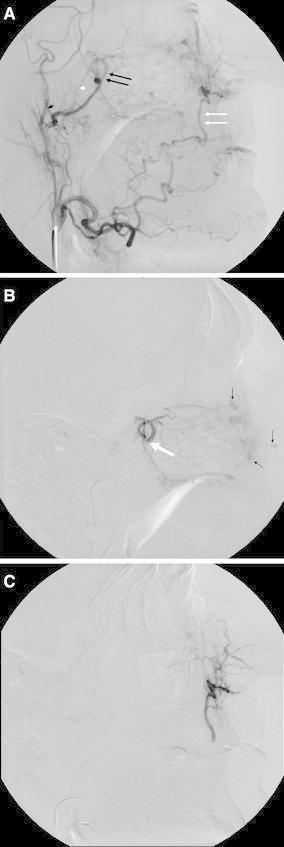
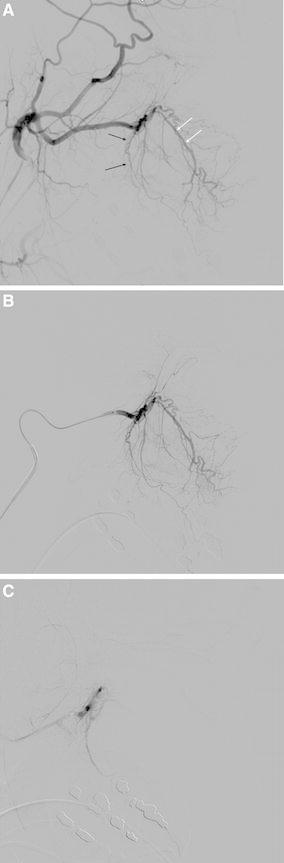
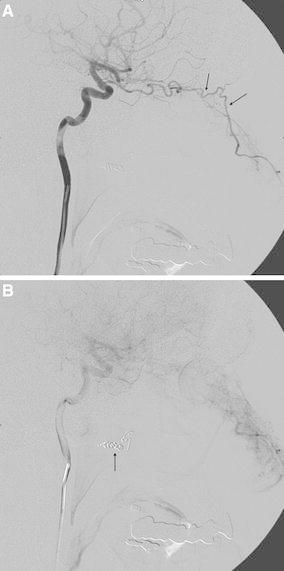
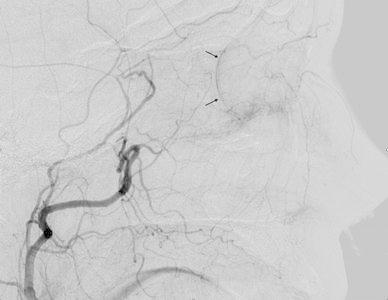
The majority of episodes of spontaneous posterior epistaxis treated with embolisation are idiopathic in nature. The angiographic findings are typically normal. Specific angiographic signs are rare and may include the following: a tumour blush, telangiectasia, aneurysm, and/or extravasation. Selective internal carotid artery (ICA) angiography may show rare causes of epistaxis, such as traumatic or mycotic aneurysms, which require different treatment approaches. Complete bilateral selective external and internal carotid angiograms are essential to evaluation. The images should be analysed for detection of central retinal blush in the external carotid artery (ECA) and anastomoses between the branches of the ECA and ICA. Monocular blindness and stroke are two of the most severe complications. Embolisation aims to decrease flow to the bleeding nasal mucosa while avoiding necrosis of the nasal skin and palate mucosa. Embolisation is routinely performed with a microcatheter positioned in the internal maxillary artery distal to the origin of the meningeal arteries. A guiding catheter should be placed in the proximal portion of the ECA to avoid vasospasm. Embolisation with microparticles is halted when the peripheral branches of the sphenopalatine artery are occluded. The use of coils is not recommended because recurrent epistaxis may occur due to proximal embolization; moreover, the option of repeat distal embolisation is lost. The success rate of embolisation therapy (accounting for late recurrence of bleeding) varies between 71 and 94 %. Results from endoscopic surgery are quite comparable. When epistaxis is refractory to nasal packing or endoscopic surgery, embolisation is the treatment of choice in some centres.
Figures
References
-
- Shukla PA, Chan N, Duffis EJ, Eloy JA, Prestigiacomo CJ, Gandhi CD. Current treatment strategies for epistaxis: a multidisciplinary approach. J Neurointerv Surg. 2012;5(2):1–6. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
