

Optimization of near-infrared fluorescence cholangiography for open and laparoscopic surgery
- PMID: 24232054
- PMCID: PMC4021038
- DOI: 10.1007/s00464-013-3305-9
Optimization of near-infrared fluorescence cholangiography for open and laparoscopic surgery
Abstract
Background: During laparoscopic cholecystectomy, common bile duct (CBD) injury is a rare but severe complication. To reduce the risk of injury, near-infrared (NIR) fluorescent cholangiography using indocyanine green (ICG) has recently been introduced as a novel method of visualizing the biliary system during surgery. To date, several studies have shown feasibility of this technique; however, liver background fluorescence remains a major problem during fluorescent cholangiography. The aim of the current study was to optimize ICG dose and timing for NIR cholangiography using a quantitative intraoperative camera system during open hepatopancreatobiliary (HPB) surgery. Subsequently, these results were validated during laparoscopic cholecystectomy using a laparoscopic fluorescence imaging system.
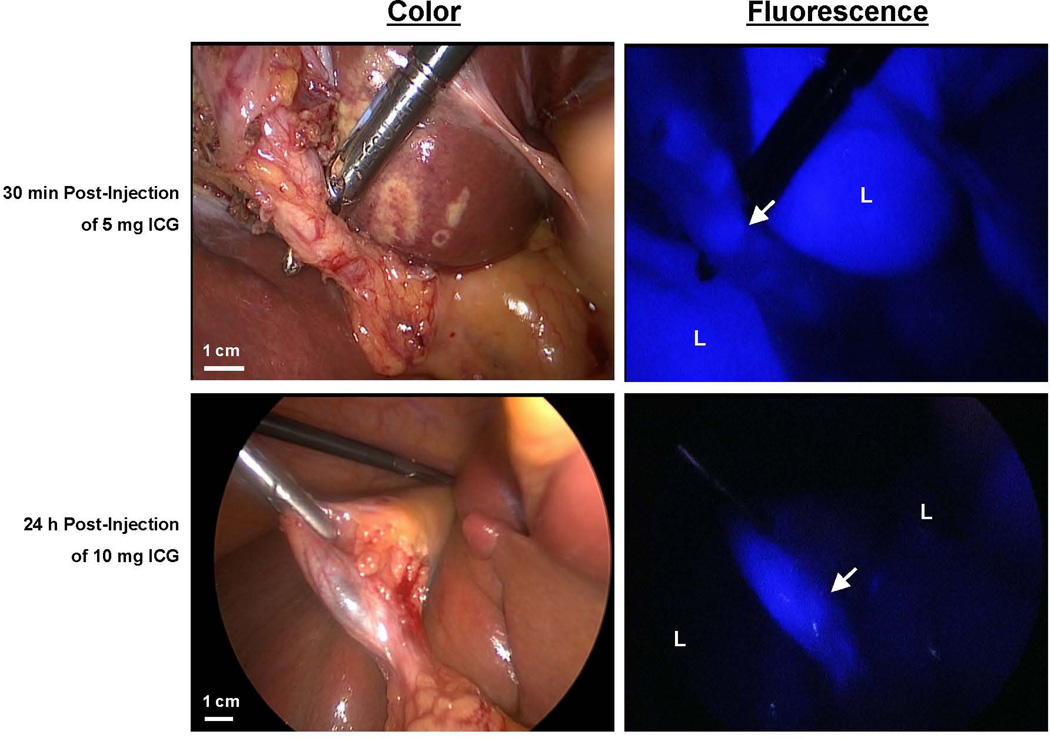
Methods: Twenty-seven patients who underwent NIR imaging using the Mini-FLARE image-guided surgery system during open HPB surgery were analyzed to assess optimal dosage and timing of ICG administration. ICG was intravenously injected preoperatively at doses of 5, 10, and 20 mg, and imaged at either 30 min (early) or 24 h (delayed) post-injection. Next, the optimal doses found for early and delayed imaging were applied to two groups of seven patients (n = 14) undergoing laparoscopic NIR fluorescent cholangiography during laparoscopic cholecystectomy.
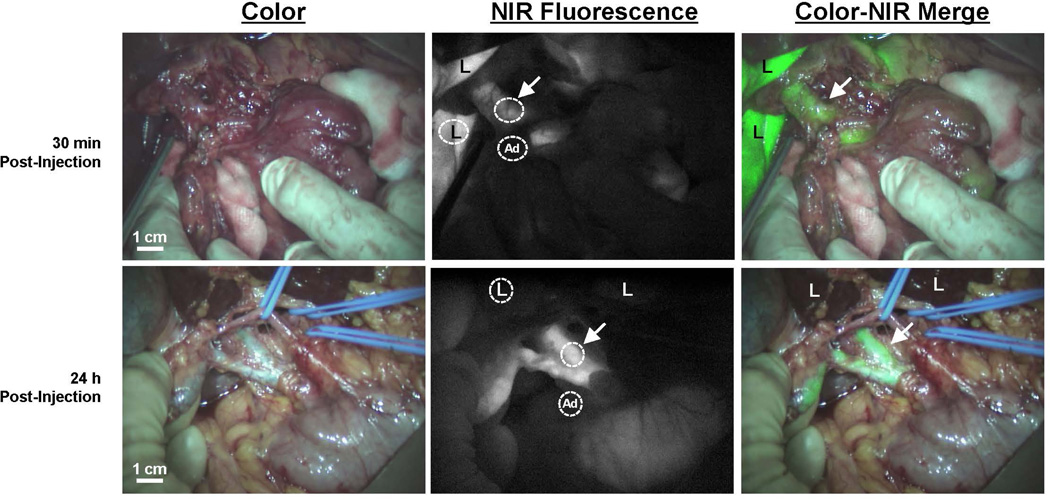
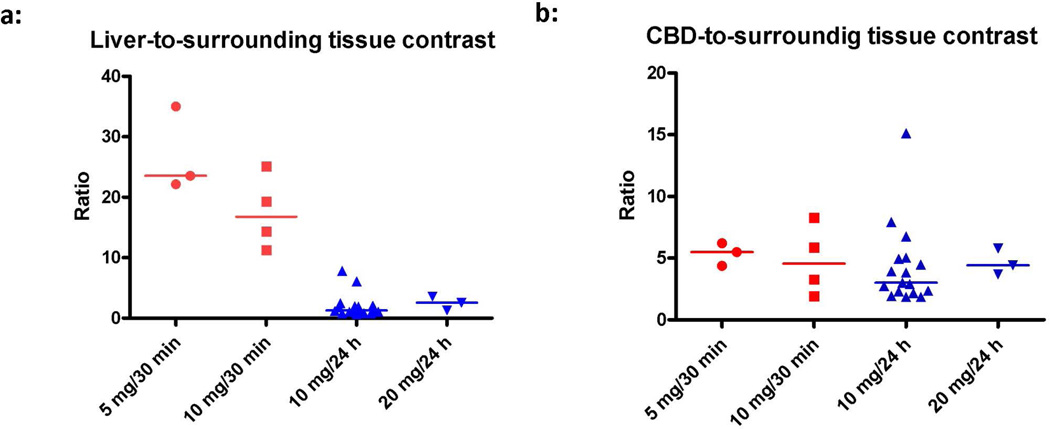
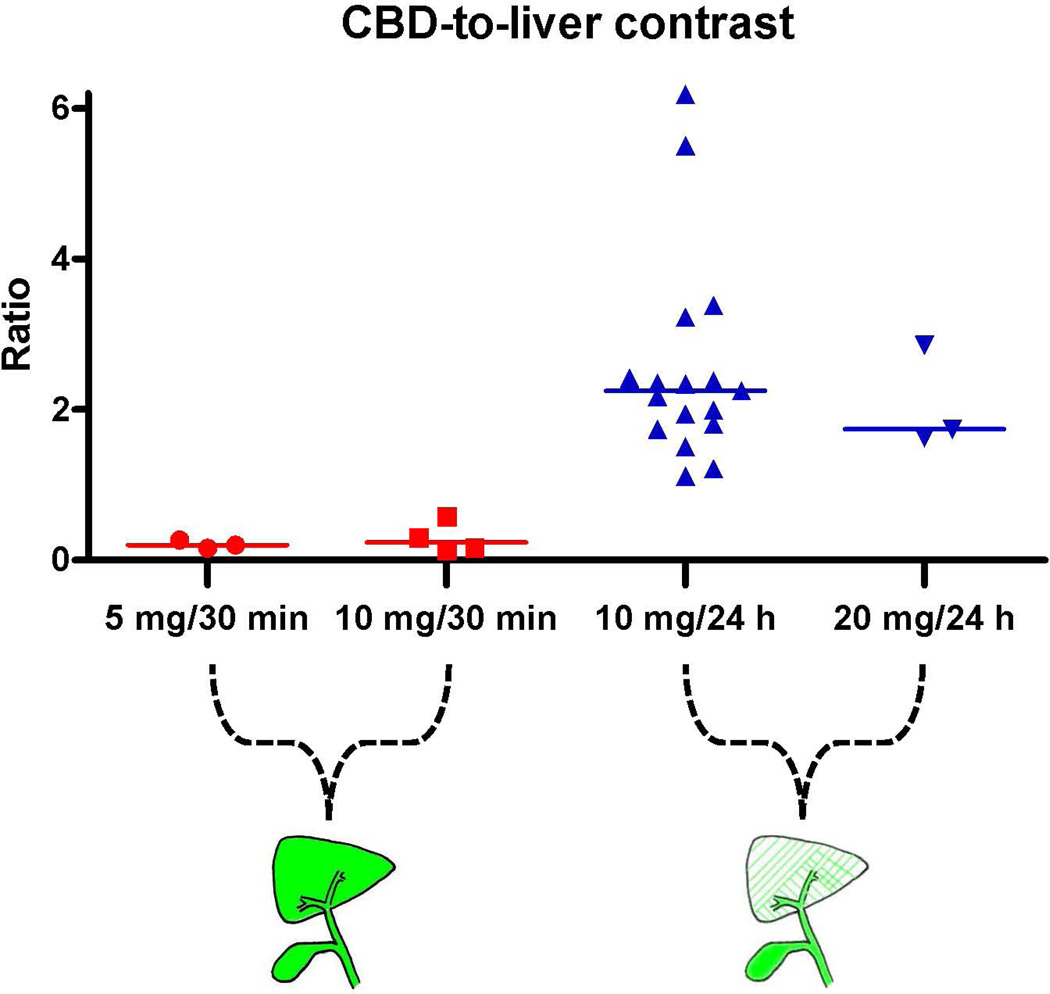
Results: Median liver-to-background contrast was 23.5 (range 22.1–35.0), 16.8 (range 11.3–25.1), 1.3 (range 0.7–7.8), and 2.5 (range 1.3–3.6) for 5 mg/30 min, 10 mg/30 min, 10 mg/24 h, and 20 mg/24 h, respectively. Fluorescence intensity of the liver was significantly lower in the 10 mg delayed-imaging dose group compared with the early imaging 5 and 10 mg dose groups (p = 0.001), which resulted in a significant increase in CBD-to-liver contrast ratio compared with the early administration groups (p < 0.002). These findings were qualitatively confirmed during laparoscopic cholecystectomy.
Conclusion: This study shows that a prolonged interval between ICG administration and surgery permits optimal NIR cholangiography with minimal liver background fluorescence.
Conflict of interest statement
F.P.R. Verbeek, B.E. Schaafsma, Q.R.J.G. Tummers, J.R. van der Vorst, W.J. van der Made, C.I. Baeten, B.A. Bonsing, C.J.H. van de Velde, A.L. Vahrmeijer and R.J. Swijnenburg have no conflicts of interest or financial ties to disclose.
Figures
References
-
- NIH Consensus conference. Gallstones and laparoscopic cholecystectomy. JAMA. 1993;269:1018–1024. - PubMed
-
- Perissat J. Laparoscopic cholecystectomy: the European experience. Am J Surg. 1993;165:444–449. - PubMed
-
- Deziel DJ, Millikan KW, Economou SG, Doolas A, Ko ST, Airan MC. Complications of laparoscopic cholecystectomy: a national survey of 4,292 hospitals and an analysis of 77,604 cases. Am J Surg. 1993;165:9–14. - PubMed
-
- Flum DR, Koepsell T, Heagerty P, Sinanan M, Dellinger EP. Common bile duct injury during laparoscopic cholecystectomy and the use of intraoperative cholangiography: adverse outcome or preventable error? Arch Surg. 2001;136:1287–1292. - PubMed
-
- Giger U, Ouaissi M, Schmitz SF, Krahenbuhl S, Krahenbuhl L. Bile duct injury and use of cholangiography during laparoscopic cholecystectomy. Br J Surg. 2011;98:391–396. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
