

The economic value of personalized medicine tests: what we know and what we need to know
- PMID: 24232413
- PMCID: PMC3949119
- DOI: 10.1038/gim.2013.122
The economic value of personalized medicine tests: what we know and what we need to know
Abstract
Purpose: There is uncertainty about when personalized medicine tests provide economic value. We assessed evidence on the economic value of personalized medicine tests and gaps in the evidence base.
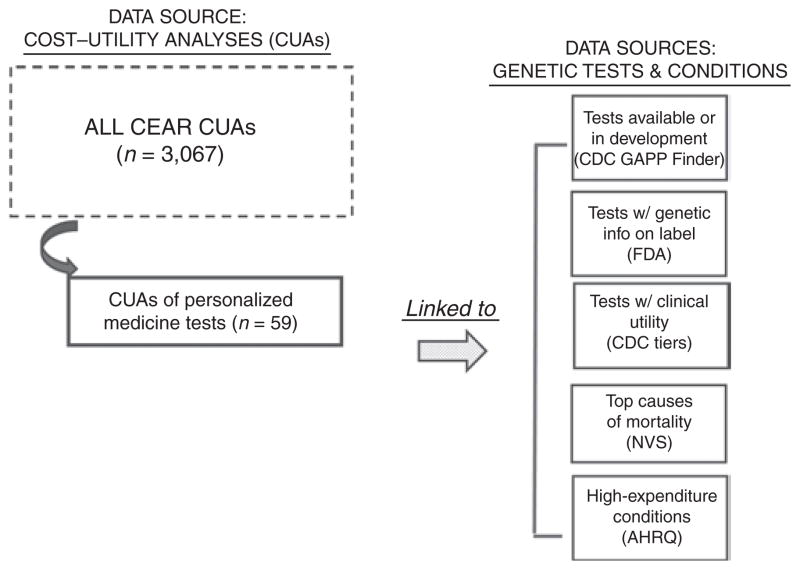
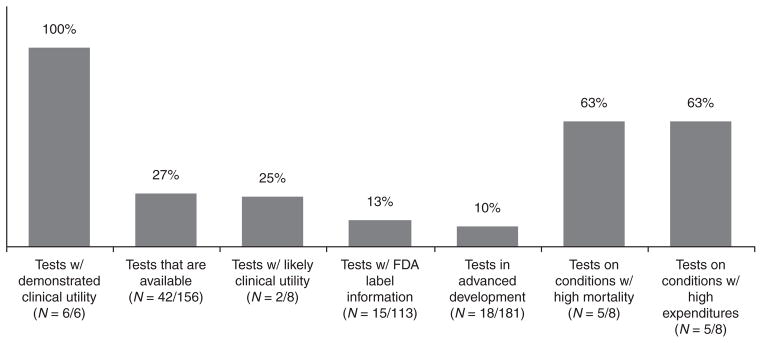
Methods: We created a unique evidence base by linking data on published cost-utility analyses from the Tufts Cost-Effectiveness Analysis Registry with data measuring test characteristics and reflecting where value analyses may be most needed: (i) tests currently available or in advanced development, (ii) tests for drugs with Food and Drug Administration labels with genetic information, (iii) tests with demonstrated or likely clinical utility, (iv) tests for conditions with high mortality, and (v) tests for conditions with high expenditures.
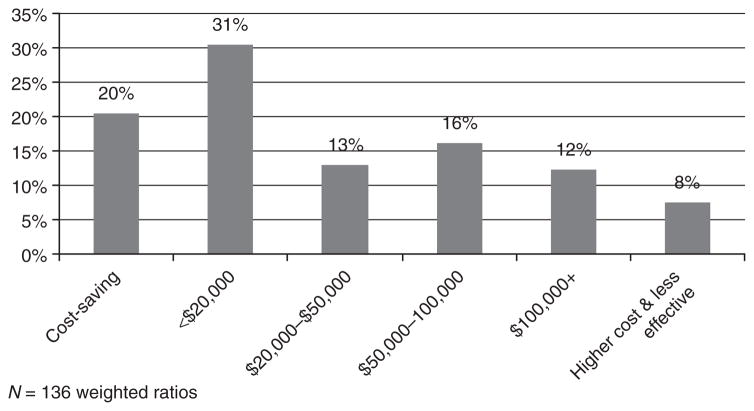
Results: We identified 59 cost-utility analyses studies that examined personalized medicine tests (1998-2011). A majority (72%) of the cost/quality-adjusted life year ratios indicate that testing provides better health although at higher cost, with almost half of the ratios falling below $50,000 per quality-adjusted life year gained. One-fifth of the results indicate that tests may save money.
Conclusion: Many personalized medicine tests have been found to be relatively cost-effective, although fewer have been found to be cost saving, and many available or emerging medicine tests have not been evaluated. More evidence on value will be needed to inform decision making and assessment of genomic priorities.
Conflict of interest statement
DISCLOSURE
The authors declare no conflict of interest.
Figures
Comment in
-
Economic analyses of genetic tests in personalized medicine: clinical utility first, then cost utility.Genet Med. 2014 Mar;16(3):225-7. doi: 10.1038/gim.2013.158. Epub 2013 Oct 10. Genet Med. 2014. PMID: 24232411 Free PMC article. No abstract available.
References
-
- Armstrong K. Can genomics bend the cost curve? JAMA. 2012;307:1031–1032. - PubMed
-
- [Accessed 10 December, 2012];Clinically Relevant Genetic Variants Resource: A Unified Approach for Identifying Genetic Variants for Clinical Use (U01) http://grants.nih.gov/grants/guide/rfafiles/rfa-hg-12-016.html.
-
- Cohen JT, Neumann PJ, Weinstein MC. Does preventive care save money? Health economics and the presidential candidates. N Engl J Med. 2008;358:661– 663. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
