

Diagnosis, management, and long-term outcomes of rectovaginal endometriosis
- PMID: 24232977
- PMCID: PMC3825702
- DOI: 10.2147/IJWH.S37846
Diagnosis, management, and long-term outcomes of rectovaginal endometriosis
Abstract
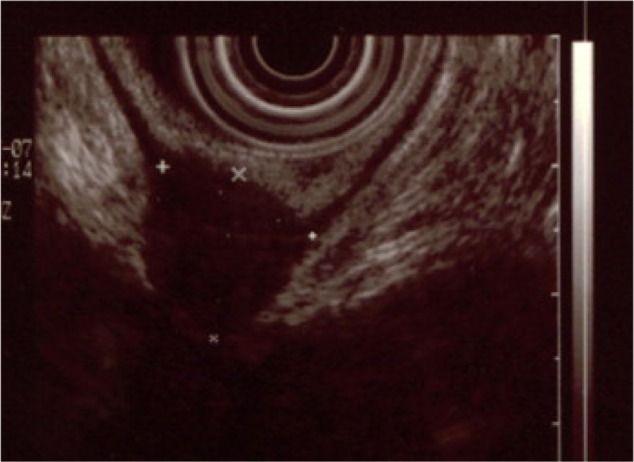
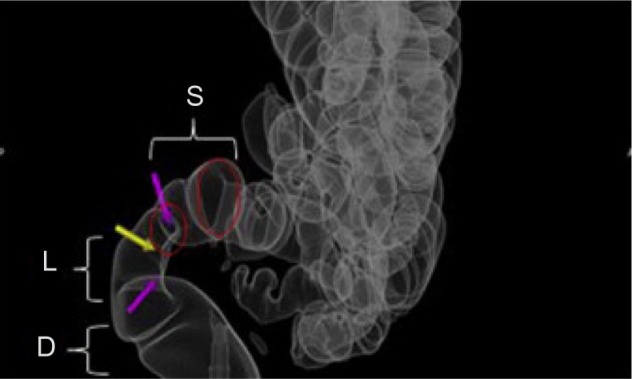
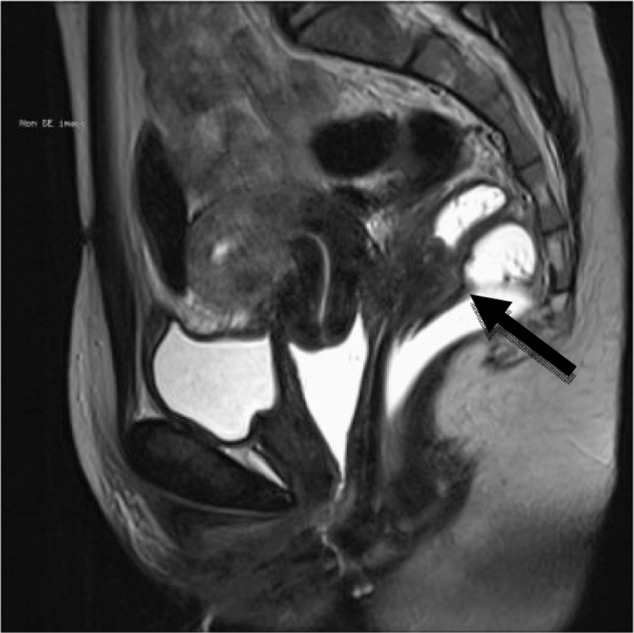
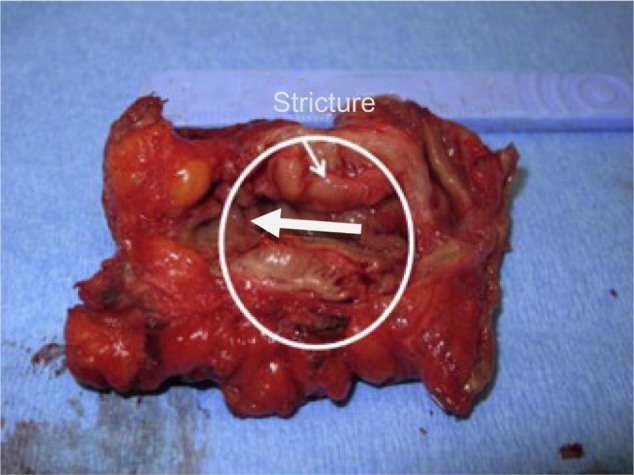
Rectovaginal endometriosis is the most severe form of endometriosis. Clinically, it presents with a number of symptoms including chronic pelvic pain, dysmenorrhea, deep dyspareunia, dyschezia, and rectal bleeding. The gold standard for diagnosis is laparoscopy with histological confirmation; however, there are a number of options for presurgical diagnosis, including clinical examination, transvaginal/transrectal ultrasound, magnetic resonance imagining, colonoscopy, and computed tomography colonography. Treatment can be medical or surgical. Medical therapies include birth control pills, oral progestins, gonadotropin-releasing hormone agonists, danazol, and injectable progestins. Analgesics are often used as well. Surgery improves up to 70% of symptoms. Surgery is either ablative or excisional, and is conducted via transvaginal, laparoscopic, laparotomy, or combined approaches. Common surgical techniques involve shaving of the superficial rectal lesion, laparoscopic anterior discoid resection, and low anterior bowel resection and reanastomosis. Outcomes are generally favorable, but postoperative complications may include intra-abdominal bleeding, anastomotic leaks, rectovaginal fistulas, strictures, chronic constipation, and the need for reoperation. Recurrence of rectal endometriosis is a possibility as well. Other outcomes are improved pain-related symptoms and fertility. Long-term outcomes vary according to the management strategy used. This review will provide the most recent approaches and techniques for the diagnosis and treatment of rectovaginal endometriosis.
Keywords: bowel resection; dyspareunia; endometriosis; pelvic pain; rectovaginal.
Figures
References
-
- Roberts CP, Rock JA. The current staging system for endometriosis: does it help? Obstet Gynecol Clin North Am. 2003;30(1):115–132. - PubMed
-
- Tarjanne S, Sjöberg J, Heikinheimo O. Rectovaginal endometriosis-characteristics of operative treatment and factors predicting bowel resection. J Minim Invasive Gynecol. 2009;16(3):302–306. - PubMed
-
- Zanetti-Dällenbach R, Bartley J, Müller C, Schneider A, Köhler C. Combined vaginal-laparoscopic-abdominal approach for the surgical treatment of rectovaginal endometriosis with bowel resection: a comparison of this new technique with various established approaches by laparoscopy and laparotomy. Surg Endosc. 2008;22(4):995–1001. - PubMed
-
- Kondo W, Branco AW, Trippia CH, Ribeiro R, Zomer MT. Retrocervical deep infiltrating endometriotic lesions larger than thirty millimeters are associated with an increased rate of ureteral involvement. J Minim Invasive Gynecol. 2013;20(1):100–103. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
