

Implementation of high-resolution manometry in the clinical practice of speech language pathology
- PMID: 24233810
- PMCID: PMC4201623
- DOI: 10.1007/s00455-013-9494-5
Implementation of high-resolution manometry in the clinical practice of speech language pathology
Abstract
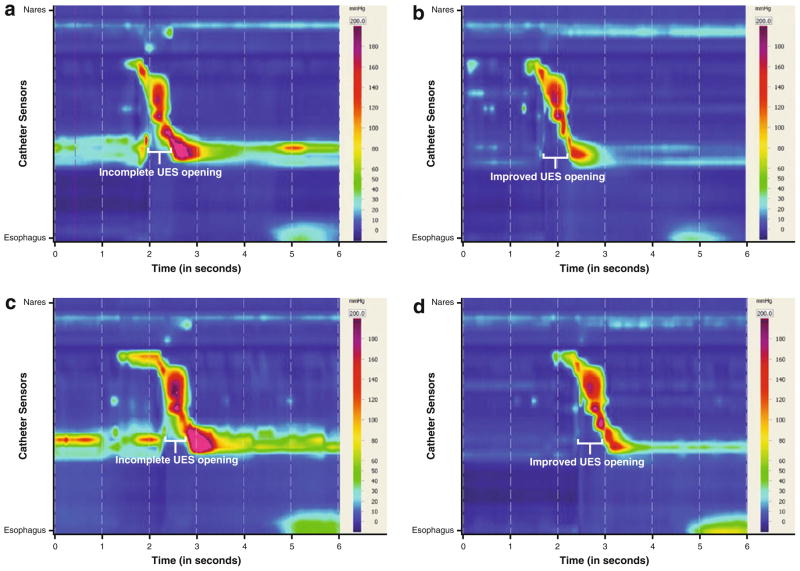
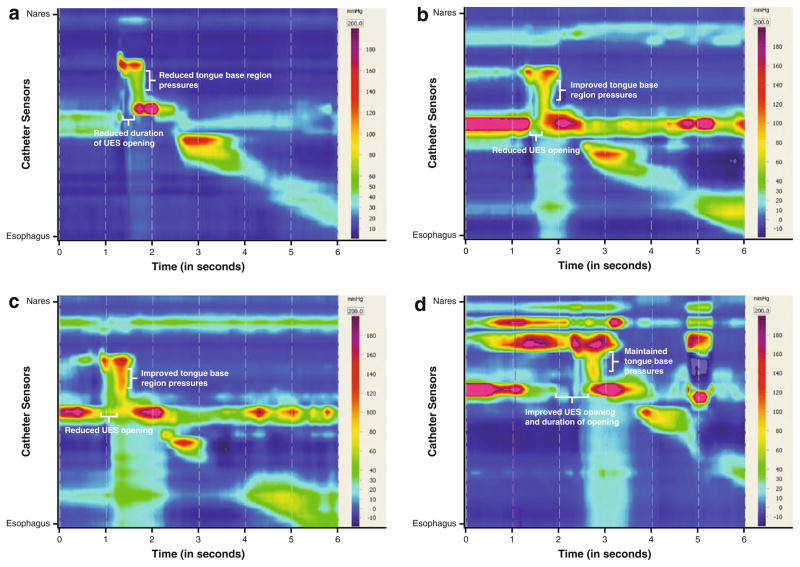
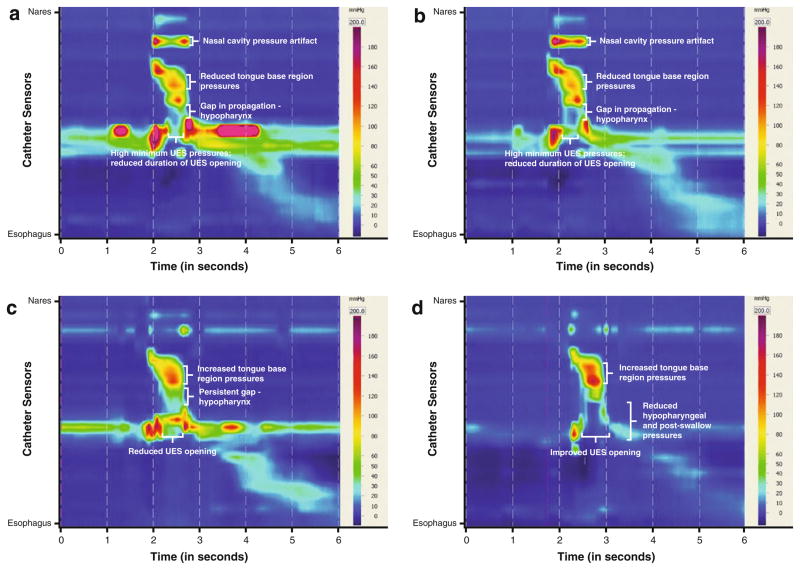
Visual imaging modalities, videofluoroscopic swallow study (VFSS) and fiberoptic endoscopic evaluation of swallow, for assessment of oropharyngeal dysphagia have been part of the speech language pathologist's (SLPs) armamentarium for the diagnosis and treatment of dysphagia for decades. Recently, the addition of high-resolution manometry (HRM) has enabled the SLP to evaluate pharyngeal pressures and upper esophageal sphincter relaxation. Taken together, the use of visual imaging modalities with HRM can improve interpretation of swallowing physiology and facilitate more effective treatment planning. The goal of this article is to describe a clinical paradigm using HRM as an adjunct to VFSS, by the SLP, in the assessment of complex dysphagia. Moreover, in three cases described, the value of manometric measurements in elucidating swallowing imaging studies and documenting physiologic change in response to treatment is highlighted. As technology in this area is evolving, so will the clinical use of HRM by the SLP. Limitations of current HRM systems and applications are discussed.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures



References
-
- Rosenbek JC, Robbins JA, Roecker EB, et al. A penetration–aspiration scale. Dysphagia. 1996;11:93–8. - PubMed
-
- Aviv JE. Prospective, randomized outcome study of endoscopy versus modified barium swallow in patients with dysphagia. Laryngoscope. 2000;110:563–74. - PubMed
-
- Kelly AM, Drinnan MJ, Leslie P. Assessing penetration and aspiration: how do videofluoroscopy and fiberoptic endoscopic evaluation of swallowing compare? Laryngoscope. 2007;117:1723–7. - PubMed
-
- Colodny N. Interjudge and intrajudge reliabilities in fiberoptic endoscopic evaluation of swallowing (FEES) using the penetration–aspiration scale: a replication study. Dysphagia. 2002;17:308–15. - PubMed
-
- Kuhlemeier KV, Yates P, Palmer JB. Intra- and interrater variation in the evaluation of videofluorographic swallowing studies. Dysphagia. 1998;13:142–7. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
