Management of secondary pelviureteric junction obstruction
- PMID: 24235791
- PMCID: PMC3822345
- DOI: 10.4103/0970-1591.120110
Management of secondary pelviureteric junction obstruction
Abstract
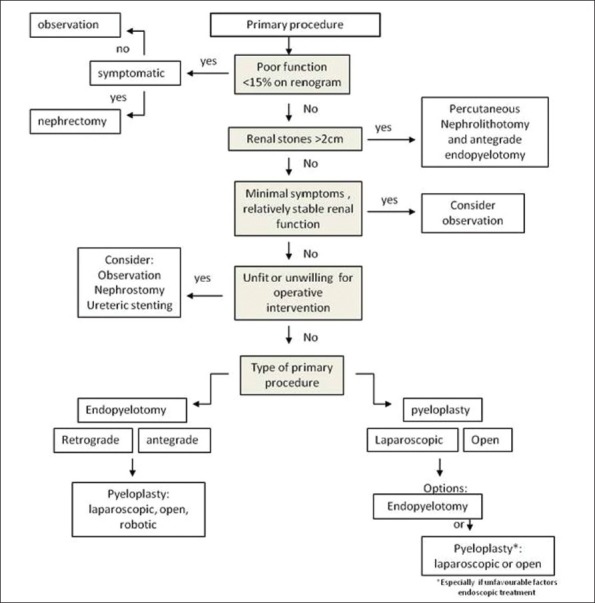
Pelviureteric junction obstruction (PUJO) of the kidney can lead to a number of different clinical manifestations, which often require surgical intervention. Although the success of pyeloplasty and endopyelotomy are good, there are still a number of patients who fail primary treatment and develop secondary PUJO. These treatment failures can be a challenging cohort to manage. This article aims to provide a comprehensive overview on the surgical options available to the urologist for managing secondary PUJO as well as providing some guidance on assessing factors that will influence management decisions.
Keywords: Endopyelotomy; laparoscopic pyeloplasty; pelviureteric junction obstruction; reconstruction.
Conflict of interest statement
Figures
References
-
- Rassweiler JJ, Subotic S, Feist-Schwenk M, Sugiono M, Schulze M, Teber D, et al. Minimally invasive treatment of ureteropelvic junction obstruction: Long-term experience with an algorithm for laser endopyelotomy and laparoscopic retroperitoneal pyeloplasty. J Urol. 2007;177:1000–5. - PubMed
-
- Anderson JC, Hynes W. Retrocaval ureter: A case diagnosed pre-operatively and treated successfully by a plastic operation. Br J Urol. 1949;21:209–14. - PubMed
-
- Webber RJ, Pandian SS, McClinton S, Hussey J. Retrograde balloon dilatation for pelviureteric junction obstruction: Long-term follow-up. J Endourol. 1997;11:239–42. - PubMed
-
- Schuessler WW, Grune MT, Tecuanhuey LV, Preminger GM. Laparoscopic dismembered pyeloplasty. J Urol. 1993;150:1795–9. - PubMed
-
- Jarrett TW, Chan DY, Charambura TC, Fugita O, Kavoussi LR. Laparoscopic pyeloplasty: The first 100 cases. J Urol. 2002;167:1253–6. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources