

Randomised clinical trial: individualised vs. weight-based dosing of azathioprine in Crohn's disease
- PMID: 24237037
- PMCID: PMC3918445
- DOI: 10.1111/apt.12555
Randomised clinical trial: individualised vs. weight-based dosing of azathioprine in Crohn's disease
Abstract
Background: Azathioprine (AZA), a pro-drug metabolised to the active metabolites 6-tioguanine nucleotides (6TGN), is a steroid-sparing therapy for Crohn's disease (CD).
Aim: To investigate whether AZA therapy is optimised by individualised dosing based on thiopurine methyltransferase (TPMT) activity and 6TGN concentrations.
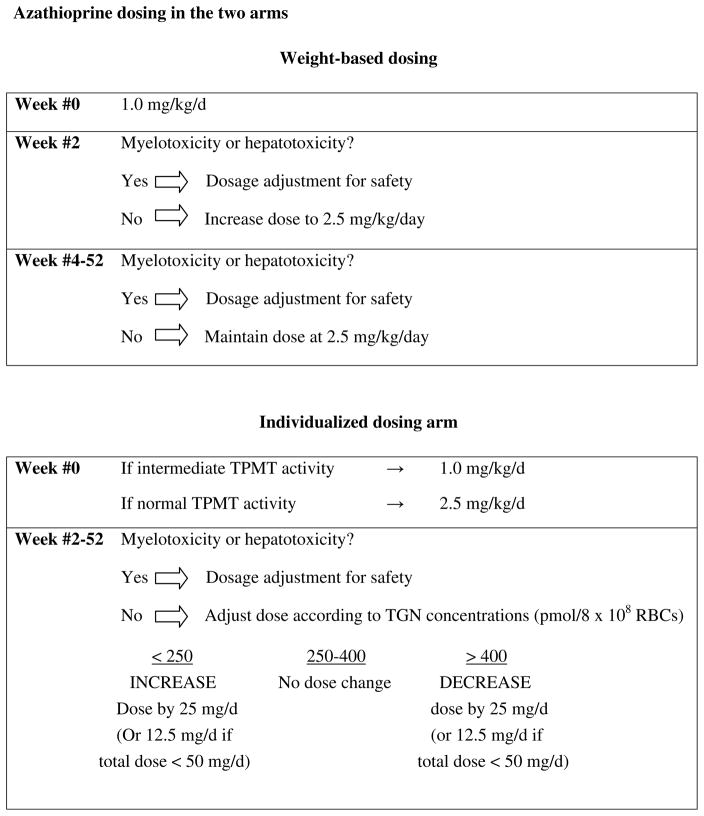
Methods: This multicentre, double-blind, randomised controlled trial compared the efficacy and safety of weight-based vs. individualised AZA dosing in inducing and maintaining remission in adults and children with steroid-treated CD. The primary outcome was clinical remission (CR) at 16 weeks. In the weight-based arm, subjects received 2.5 mg/kg/day. In the individualised dosing arm, the initial AZA dose was 1.0 mg/kg/day (if intermediate TPMT) or 2.5 mg/kg/day (if normal TPMT). Starting at week 5, the dose was adjusted to target 6TGN concentrations of 250-400 pmol/8 × 10(8) red blood cells (RBC), or to a maximal dose of 4 mg/kg/day.
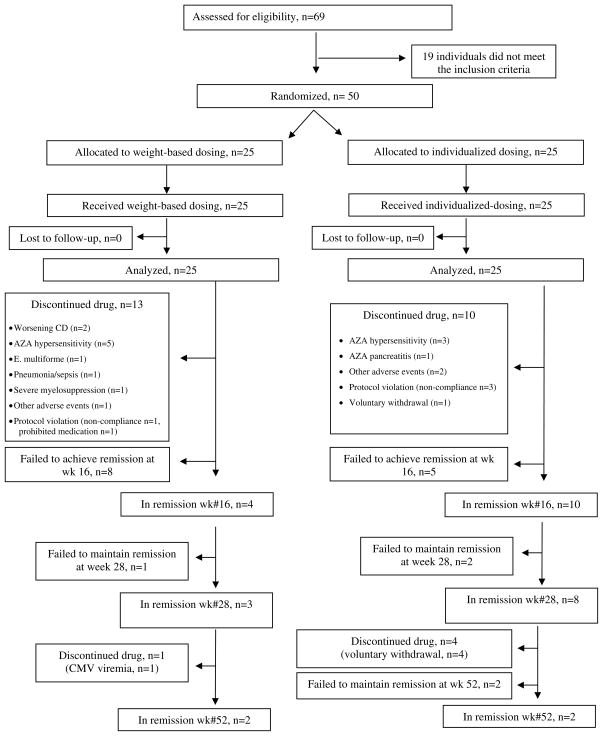
Results: After randomising 50 subjects, the trial was stopped prematurely due to insufficient enrolment. In intention-to-treat analysis, CR rates at week 16 were 40% in the individualised arm vs. 16% in the weight-based arm (P = 0.11). In per-protocol (PP) analysis, week 16 CR rates were 60% in the individualised arm and 25% in the weight-based arm (P = 0.12). At week 16, median 6TGN concentrations in PP remitters and nonremitters were 216 and 149 pmol/8 × 10(8) RBC respectively (P = 0.07).
Conclusions: Despite trends favouring individualised over weight-based AZA dosing, there were no statistically significant differences in efficacy, likely due to low statistical power and inability to achieve the target 6TGN concentrations in the individualised arm. [Clinicaltrials.Gov Identifier Nct00113503].
Trial registration: ClinicalTrials.gov NCT00113503.
© 2013 John Wiley & Sons Ltd.
Figures
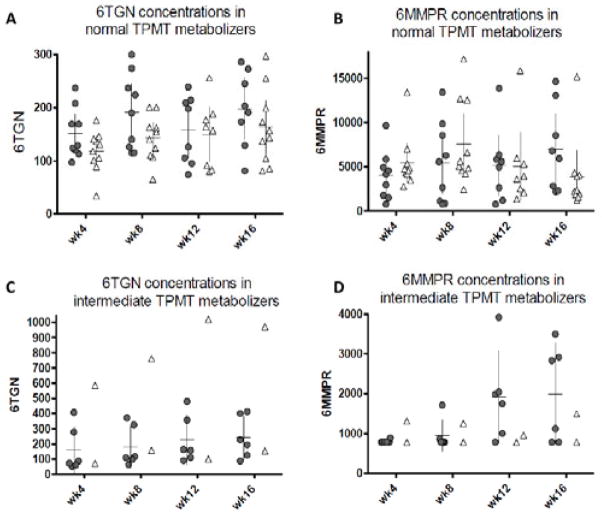
 ) and in the weight-based arm (Δ) (per protocol analysis). A: 6TGN concentrations in normal metabolizers. B: 6MMPR concentrations in normal metabolizers. C: 6TGN concentrations in intermediate metabolizes. D: 6MMPR concentrations in intermediate metabolizes.
) and in the weight-based arm (Δ) (per protocol analysis). A: 6TGN concentrations in normal metabolizers. B: 6MMPR concentrations in normal metabolizers. C: 6TGN concentrations in intermediate metabolizes. D: 6MMPR concentrations in intermediate metabolizes.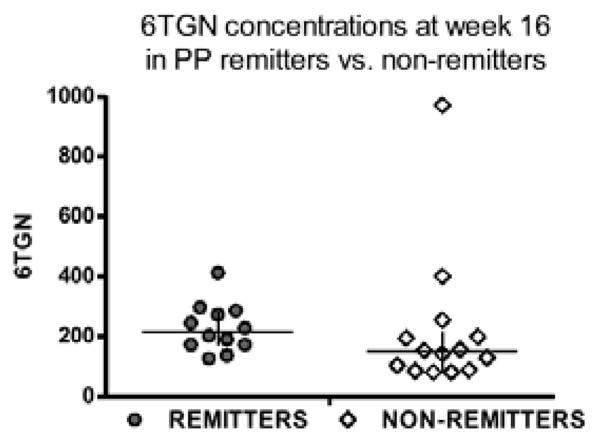
Comment in
-
Commentary: Individual vs. weight-based dosing of azathioprine in Crohn's disease.Aliment Pharmacol Ther. 2014 Feb;39(4):438-9. doi: 10.1111/apt.12588. Aliment Pharmacol Ther. 2014. PMID: 24447314 No abstract available.
-
Letter: metabolite monitoring for thiopurines in Crohn's disease - still not fully understood.Aliment Pharmacol Ther. 2014 Mar;39(6):642. doi: 10.1111/apt.12632. Aliment Pharmacol Ther. 2014. PMID: 24588251 No abstract available.
References
-
- Prefontaine E, Sutherland LR, Macdonald JK, Cepoiu M. Azathioprine or 6-mercaptopurine for maintenance of remission in Crohn’s disease. Cochrane Database Syst Rev. 2009;(1):CD000067. - PubMed
-
- Dignass A, Van Assche G, Lindsay JO, et al. The second European evidence-based Consensus on the diagnosis and management of Crohn’s disease: Current management. J Crohns Colitis. 2010;4(1):28–62. - PubMed
-
- Talley NJ, Abreu MT, Achkar JP, et al. An evidence-based systematic review on medical therapies for inflammatory bowel disease. Am J Gastroenterol. 2011;106 (Suppl 1):S2–25. - PubMed
-
- Ha C, Dassopoulos T. Thiopurine therapy in inflammatory bowel disease. Expert Rev Gastroenterol Hepatol. 2010;4(5):575–88. - PubMed
-
- Colombel JF, Ferrari N, Debuysere H, et al. Genotypic analysis of thiopurine S-methyltransferase in patients with Crohn’s disease and severe myelosuppression during azathioprine therapy. Gastroenterology. 2000;118(6):1025–30. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous