

The Ask-Advise-Connect approach for smokers in a safety net healthcare system: a group-randomized trial
- PMID: 24237916
- PMCID: PMC4023543
- DOI: 10.1016/j.amepre.2013.07.011
The Ask-Advise-Connect approach for smokers in a safety net healthcare system: a group-randomized trial
Abstract
Background: Because smoking has a profound impact on socioeconomic disparities in illness and death, it is crucial that vulnerable populations of smokers be targeted with treatment. The U.S. Public Health Service recommends that all patients be asked about their smoking at every visit and that smokers be given brief advice to quit and referred to treatment.
Purpose: Initiatives to facilitate these practices include the 5A's (ask, advise, assess, assist, arrange) and Ask-Advise-Refer (AAR). Unfortunately, primary care referrals are low, and most smokers referred fail to enroll. This study evaluated the efficacy of the Ask-Advise-Connect (AAC) approach to linking smokers with treatment in a large, safety net public healthcare system.
Design: The study design was a pair-matched group-randomized trial with two treatment arms.
Setting/participants: Ten safety net clinics in Houston TX.
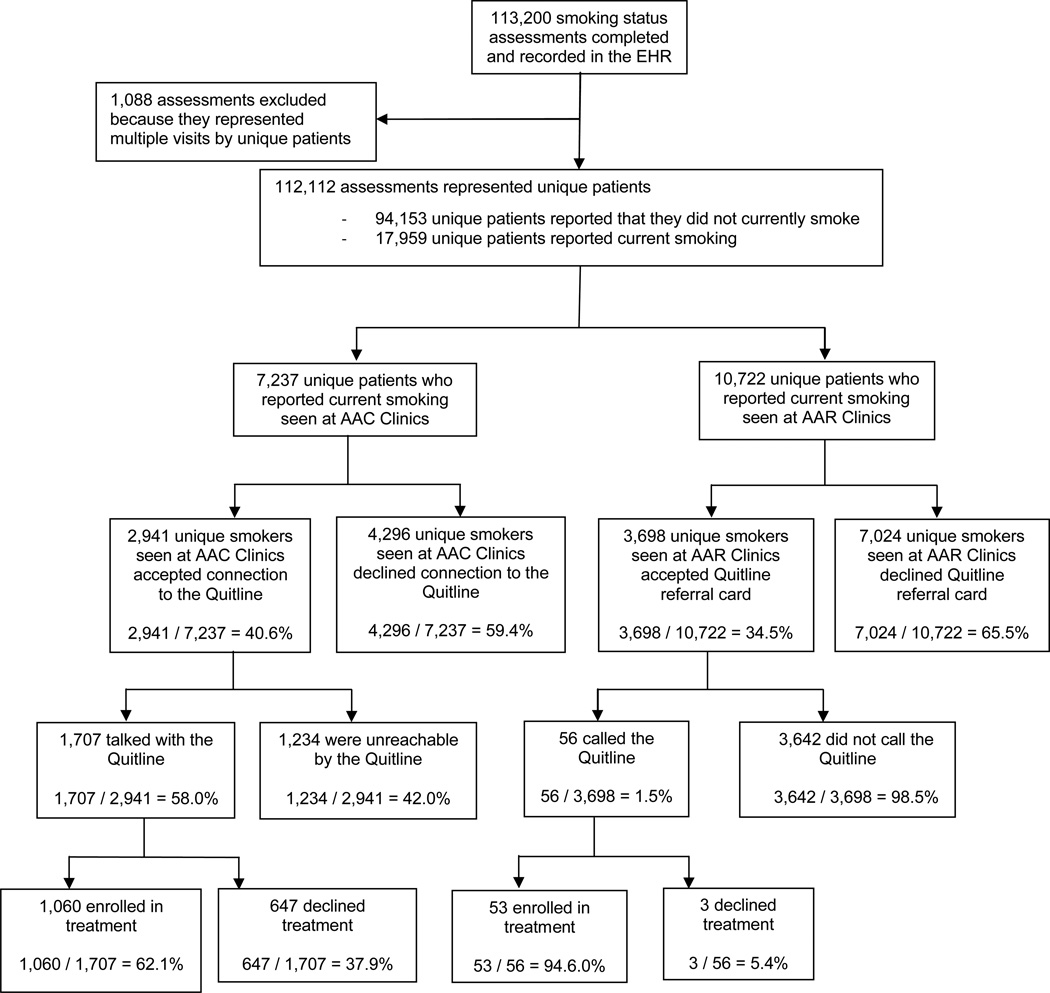
Intervention: Clinics were randomized to AAC (n=5; intervention) or AAR (n=5; control). Licensed vocational nurses (LVNs) were trained to assess and record the smoking status of all patients at all visits in the electronic health record. Smokers were given brief advice to quit. In AAC, the names and phone numbers of smokers who agreed to be connected were sent electronically to the Texas quitline daily, and patients were proactively called by the quitline within 48 hours. In AAR, smokers were offered a quitline referral card and encouraged to call on their own. Data were collected between June 2010 and March 2012 and analyzed in 2012.
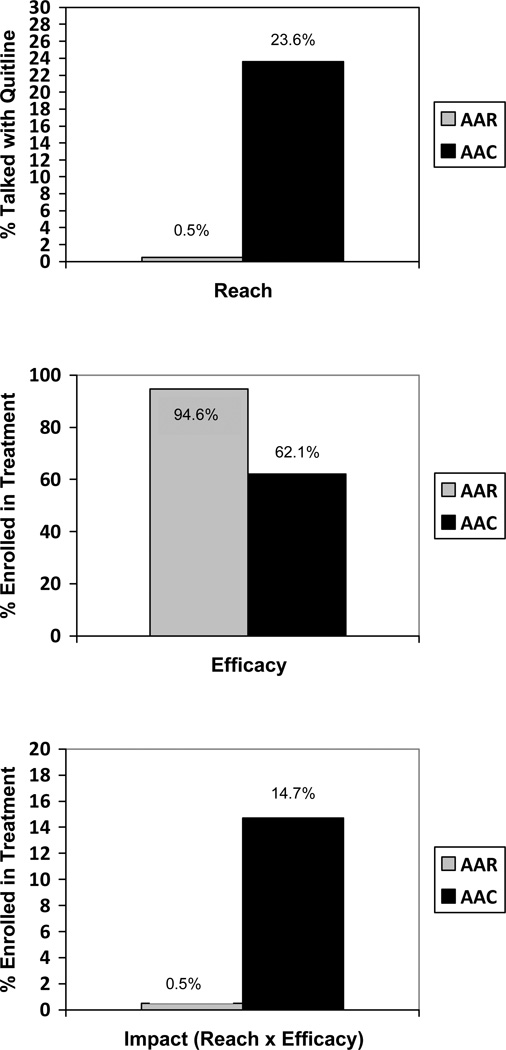
Main outcome measures: The primary outcome was impact, defined here as the proportion of identified smokers that enrolled in treatment.
Results: The impact (proportion of identified smokers who enrolled in treatment) of AAC (14.7%) was significantly greater than the impact of AAR (0.5%), t(4)=14.61, p=0.0001, OR=32.10 (95% CI=16.60, 62.06).
Conclusions: The AAC approach to aiding smoking cessation has tremendous potential to reduce tobacco-related health disparities.
© 2013 American Journal of Preventive Medicine Published by American Journal of Preventive Medicine All rights reserved.
Conflict of interest statement
Figures
References
-
- CDC. Cigarette smoking among adults - Unites States, 2000. MMWR. 2002;51:642–645. - PubMed
-
- Wetter DW, Cofta-Gunn L, Fouladi RT, et al. Understanding the associations among education, employment characteristics, and smoking. Addict Behav. 2005;30:905–914. - PubMed
-
- CDC. Cigarette smoking among adults-United States, 2003. MMWR Morb Mortal Wkly Rep. 2005;54:509–513. - PubMed
-
- Hughes JR. The future of smoking cessation therapy in the United States. Addiction. 1996;91:1797–1802. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
