

Molecular sub-group-specific immunophenotypic changes are associated with outcome in recurrent posterior fossa ependymoma
- PMID: 24240813
- PMCID: PMC3988227
- DOI: 10.1007/s00401-013-1212-8
Molecular sub-group-specific immunophenotypic changes are associated with outcome in recurrent posterior fossa ependymoma
Abstract
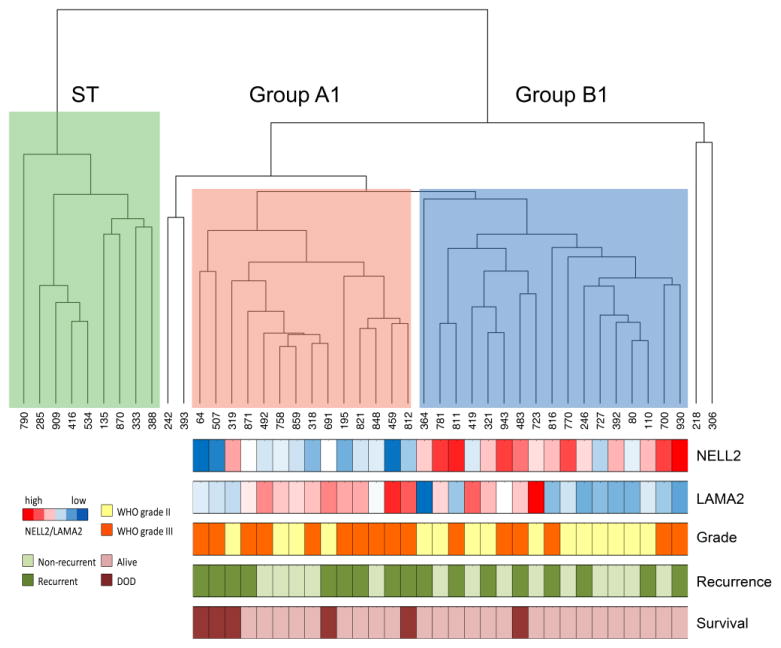
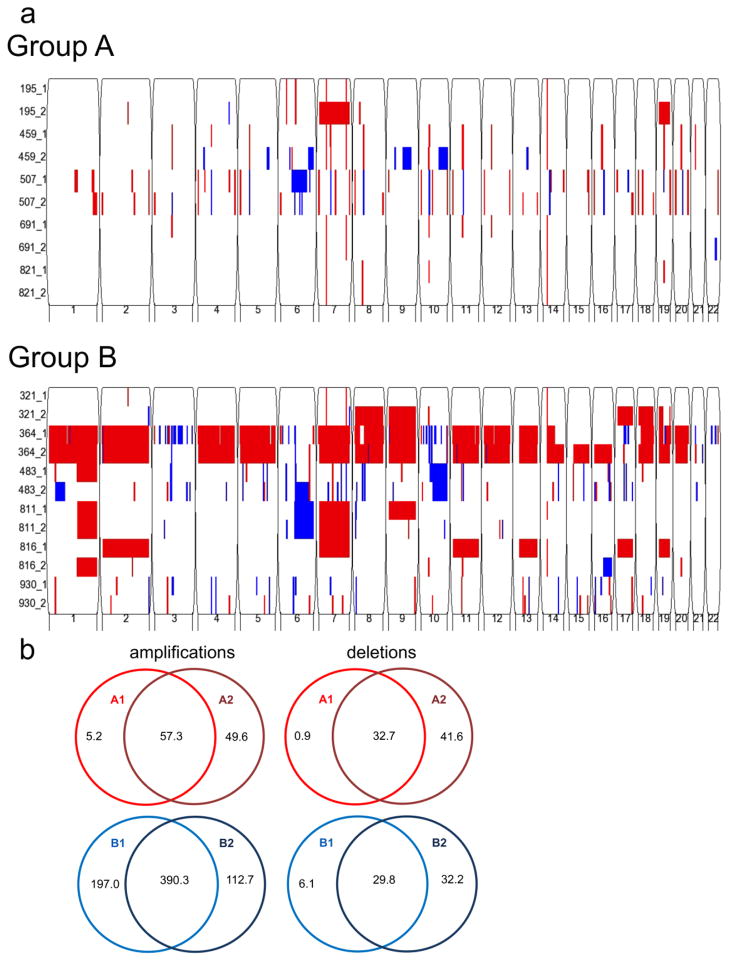
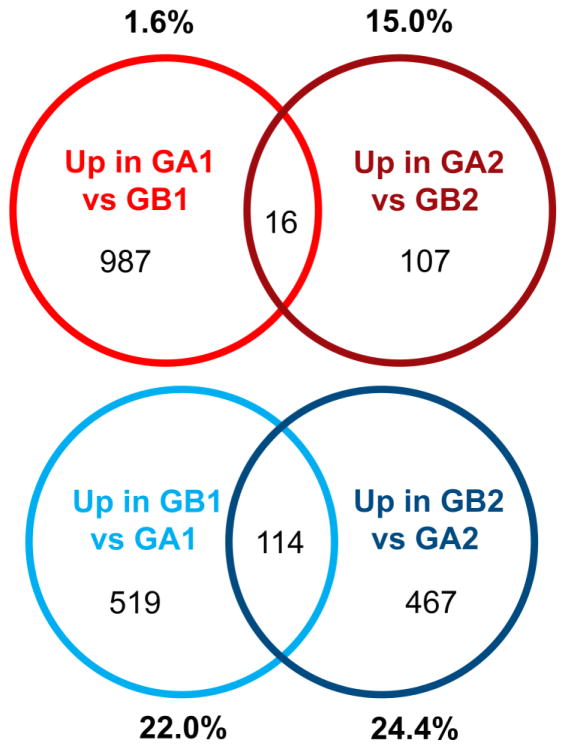
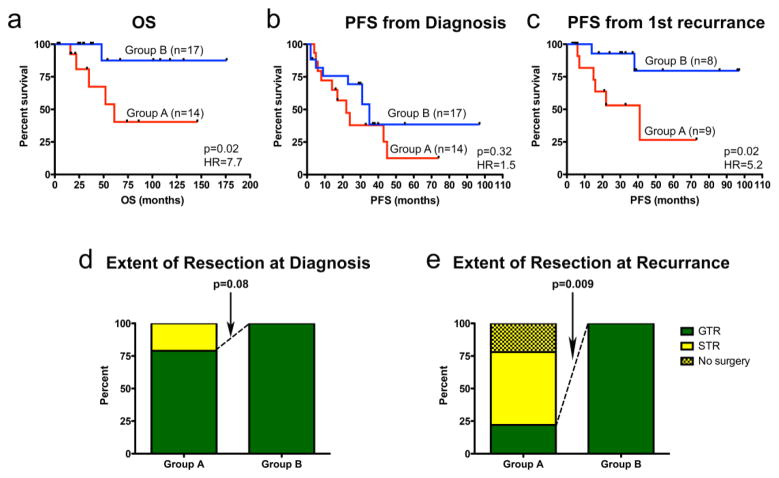
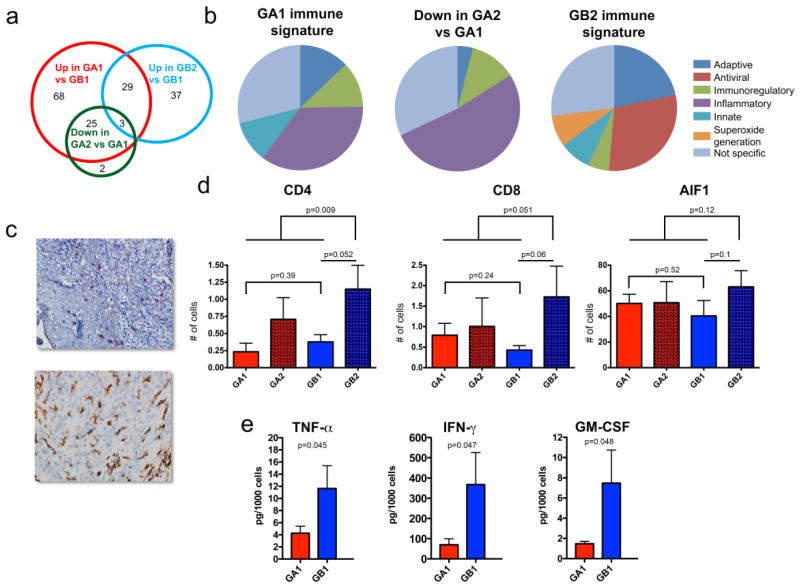
Better understanding of ependymoma (EPN) biology at relapse is needed to improve therapy at this critical event. Convincing data exist defining transcriptionally distinct posterior fossa (PF) sub-groups A and B at diagnosis. The clinical and biological consequence of these sub-groups at recurrence has not yet been defined. Genome and transcriptome microarray profiles and clinical variables of matched primary and first recurrent PF EPN pairs were used to identify biologically distinct patterns of progression between EPN sub-groups at recurrence. Key findings were validated by histology and immune function assays. Transcriptomic profiles were partially conserved at recurrence. However, 4 of 14 paired samples changed sub-groups at recurrence, and significant sub-group-specific transcriptomic changes between primary and recurrent tumors were identified, which were predominantly immune-related. Further examination revealed that Group A primary tumors harbor an immune gene signature and cellular functionality consistent with an immunosuppressive phenotype associated with tissue remodeling and wound healing. Conversely, Group B tumors develop an adaptive, antigen-specific immune response signature and increased T-cell infiltration at recurrence. Clinical distinctions between sub-groups become more apparent after first recurrence. Group A tumors were more often sub-totally resected and had a significantly shorter time to subsequent progression and worse overall survival. Minimal tumor-specific genomic changes were observed for either PF Groups A or B at recurrence. Molecular sub-groups of PF EPN convey distinct immunobiologic signatures at diagnosis and recurrence, providing potential biologic rationale to their disparate clinical outcomes. Immunotherapeutic approaches may be warranted, particularly in Group A PF EPN.
Conflict of interest statement
Figures
References
-
- Alexopoulou L, Holt AC, Medzhitov R, Flavell RA. Recognition of double-stranded RNA and activation of NF-kappaB by Toll-like receptor 3. Nature. 2001;413(6857):732–738. - PubMed
-
- Bouffet E, Perilongo G, Canete A, Massimino M. Intracranial ependymomas in children: a critical review of prognostic factors and a plea for cooperation. Med Pediatr Oncol. 1998;30(6):319–29. discussion 329–31. - PubMed
-
- Choi C, Xu X, Oh JW, Lee SJ, Gillespie GY, Park H, Jo H, Benveniste EN. Fas-induced expression of chemokines in human glioma cells: involvement of extracellular signal-regulated kinase 1/2 and p38 mitogen-activated protein kinase. Cancer Res. 2001;61(7):3084–3091. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
