

Duration of resuscitation efforts and functional outcome after out-of-hospital cardiac arrest: when should we change to novel therapies?
- PMID: 24243885
- PMCID: PMC4004337
- DOI: 10.1161/CIRCULATIONAHA.113.002408
Duration of resuscitation efforts and functional outcome after out-of-hospital cardiac arrest: when should we change to novel therapies?
Abstract
Background: Functionally favorable survival remains low after out-of-hospital cardiac arrest. When initial interventions fail to achieve the return of spontaneous circulation, they are repeated with little incremental benefit. Patients without rapid return of spontaneous circulation do not typically survive with good functional outcome. Novel approaches to out-of-hospital cardiac arrest have yielded functionally favorable survival in patients for whom traditional measures had failed, but the optimal transition point from traditional measures to novel therapies is ill defined. Our objective was to estimate the dynamic probability of survival and functional recovery as a function of resuscitation effort duration to identify this transition point.
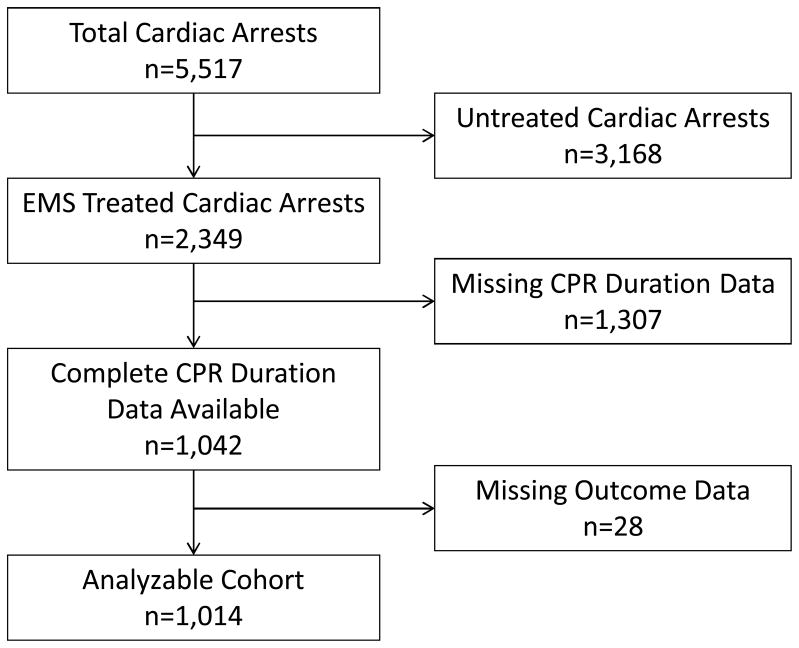
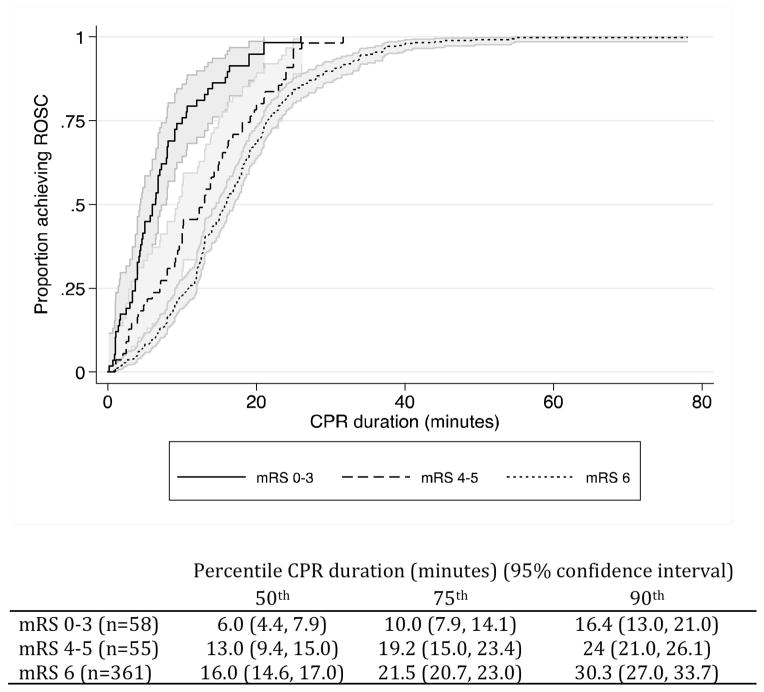
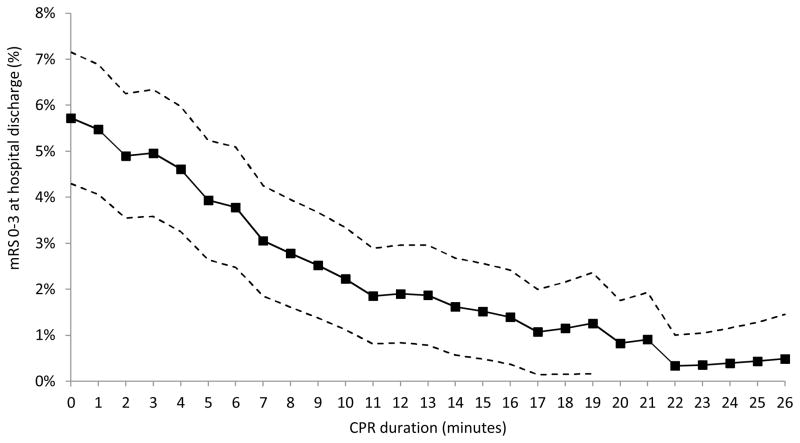
Methods and results: Retrospective cohort study of a cardiac arrest database at a single site. We included 1014 adult (≥18 years) patients experiencing nontraumatic out-of-hospital cardiac arrest between 2005 and 2011, defined as receiving cardiopulmonary resuscitation or defibrillation from a professional provider. We stratified by functional outcome at hospital discharge (modified Rankin scale). Survival to hospital discharge was 11%, but only 6% had a modified Rankin scale of 0 to 3. Within 16.1 minutes of cardiopulmonary resuscitation, 89.7% (95% confidence interval, 80.3%-95.8%) of patients with good functional outcome had achieved return of spontaneous circulation, and the probability of good functional recovery fell to 1%. Adjusting for prehospital and inpatient covariates, cardiopulmonary resuscitation duration (minutes) is independently associated with favorable functional status at hospital discharge (odds ratio, 0.84; 95% confidence interval, 0.72-0.98; P=0.02).
Conclusions: The probability of survival to hospital discharge with a modified Rankin scale of 0 to 3 declines rapidly with each minute of cardiopulmonary resuscitation. Novel strategies should be tested early after cardiac arrest rather than after the complete failure of traditional measures.
Keywords: cardiopulmonary resuscitation; heart arrest; resuscitation.
Conflict of interest statement
Figures
Comment in
-
Doing the same thing over and over, yet expecting different results.Circulation. 2013 Dec 3;128(23):2465-7. doi: 10.1161/CIRCULATIONAHA.113.005596. Epub 2013 Oct 17. Circulation. 2013. PMID: 24135072 No abstract available.
References
-
- Adielsson A, Hollenberg J, Karlsson T, Lindqvist J, Lundin S, Silfverstolpe J, Svensson L, Herlitz J. Increase in survival and bystander CPR in out-of-hospital shockable arrhythmia: bystander CPR and female gender are predictors of improved outcome. Experiences from Sweden in an 18-year perspective. Heart. 2011;97:1391–6. - PubMed
-
- Bobrow BJ, Spaite DW, Berg RA, Stolz U, Sanders AB, Kern KB, Vadeboncoeur TF, Clark LL, Gallagher JV, Stapczynski JS, LoVecchio F, Mullins TJ, Humble WO, Ewy GA. Chest compression-only CPR by lay rescuers and survival from out-of-hospital cardiac arrest. JAMA. 2010;304:1447–54. - PubMed
-
- Sunde K, Pytte M, Jacobse D, Mangschau A, Jensen LP, Smedsrud C, Draegni T, Steen PA. Implementation of a standardised treatment protocol for post resuscitation care after out-of-hospital cardiac arrest. Resuscitation. 2007;73:29–39. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
