

Lipoprotein(a) concentrations, rosuvastatin therapy, and residual vascular risk: an analysis from the JUPITER Trial (Justification for the Use of Statins in Prevention: an Intervention Trial Evaluating Rosuvastatin)
- PMID: 24243886
- PMCID: PMC3946056
- DOI: 10.1161/CIRCULATIONAHA.113.004406
Lipoprotein(a) concentrations, rosuvastatin therapy, and residual vascular risk: an analysis from the JUPITER Trial (Justification for the Use of Statins in Prevention: an Intervention Trial Evaluating Rosuvastatin)
Abstract
Background: Lipoprotein(a) [Lp(a)] is a low-density lipoprotein-like particle largely independent of known risk factors and predictive of cardiovascular disease. Statins may offset the risk associated with elevated Lp(a), but it is unknown whether Lp(a) is a determinant of residual risk in the setting of low low-density lipoprotein cholesterol after potent statin therapy.
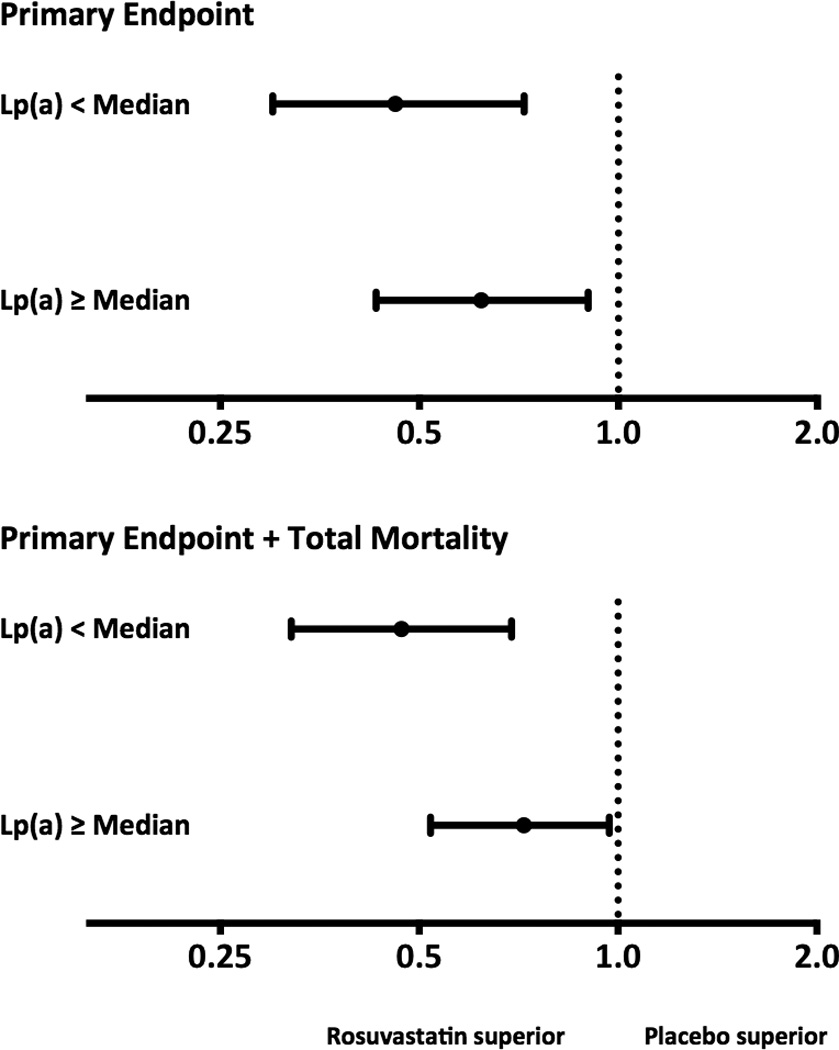
Methods and results: Baseline and on-treatment Lp(a) concentrations were assessed in 9612 multiethnic participants in the JUPITER trial (Justification for the Use of Statins in Prevention: An Intervention Trial Evaluating Rosuvastatin) before and after random allocation to rosuvastatin 20 mg/d or placebo, with outcomes reported for whites (n=7746). Lp(a) concentrations (median [25th-75th percentile], in nmol/L) were highest in blacks (60 [34-100]), then Asians (38 [18-60]), Hispanics (24 [11-46]), and whites (23 [10-50]; P<0.001). Although the median change in Lp(a) with rosuvastatin and placebo was zero, rosuvastatin nonetheless resulted in a small but statistically significant positive shift in the overall Lp(a) distribution (P<0.0001). Baseline Lp(a) concentrations were associated with incident cardiovascular disease (adjusted hazard ratio per 1-SD increment in Ln[Lp(a)], 1.18; 95% confidence interval, 1.03-1.34; P=0.02). Similarly, on-statin Lp(a) concentrations were associated with residual risk of cardiovascular disease (adjusted hazard ratio, 1.27; 95% confidence interval, 1.01-1.59; P=0.04), which was independent of low-density lipoprotein cholesterol and other factors. Rosuvastatin significantly reduced incident cardiovascular disease among participants with baseline Lp(a) greater than or equal to the median (hazard ratio, 0.62; 95% confidence interval, 0.43-0.90) and Lp(a) less than the median (hazard ratio, 0.46; 95% confidence interval, 0.30-0.72), with no evidence of interaction. Similar results were obtained when analyses included nonwhites.
Conclusion: Among white JUPITER participants treated with potent statin therapy, Lp(a) was a significant determinant of residual risk. The magnitude of relative risk reduction with rosuvastatin was similar among participants with high or low Lp(a).
Clinical trials registration url: http://www.clinicaltrials.gov. Unique identifier: NCT00239681.
Keywords: lipoproteins; risk factors; statins, HMG-CoA.
Figures
Comment in
-
Lipoprotein(a): there's life in the old dog yet.Circulation. 2014 Feb 11;129(6):619-21. doi: 10.1161/CIRCULATIONAHA.113.007256. Circulation. 2014. PMID: 24515955 No abstract available.
-
Letter by Giral et al regarding article, "lipoprotein(a) concentrations, rosuvastatin therapy, and residual vascular risk: an analysis from the JUPITER trial (justification for the use of statins in prevention: an intervention trial evaluating rosuvastatin)".Circulation. 2014 Oct 21;130(17):e151. doi: 10.1161/CIRCULATIONAHA.114.009590. Circulation. 2014. PMID: 25332284 No abstract available.
-
Response to letter regarding article, "lipoprotein(a) concentrations, rosuvastatin therapy, and residual vascular risk: an analysis from the JUPITER trial (justification for the use of statins in prevention: an intervention trial evaluating rosuvastatin)".Circulation. 2014 Oct 21;130(17):e152. doi: 10.1161/CIRCULATIONAHA.114.010927. Circulation. 2014. PMID: 25332285 No abstract available.
References
-
- Mihaylova B, Emberson J, Blackwell L, Keech A, Simes J, Barnes EH, Voysey M, Gray A, Collins R, Baigent C Cholesterol Treatment Trialists' (CTT) Collaborators. The effects of lowering LDL cholesterol with statin therapy in people at low risk of vascular disease: meta-analysis of individual data from 27 randomised trials. Lancet. 2012;380:581–590. - PMC - PubMed
-
- Tsimikas S, Hall JL. Lipoprotein(a) as a potential causal genetic risk factor of cardiovascular disease: a rationale for increased efforts to understand its pathophysiology and develop targeted therapies. J Am Coll Cardiol. 2012;60:716–721. - PubMed
-
- Berg K. A new serum type system in man—the LP system. ActaPatholMicrobiol Scand. 1963;59:369–382. - PubMed
-
- Koschinsky ML, Beisiegel U, Henne-Bruns D, Eaton DL, Lawn RM. Apolipoprotein(a) size heterogeneity is related to variable number of repeat sequences in its mRNA. Biochemistry. 1990;29:640–644. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
