

Reduction of thromboembolic events in meningioma surgery: a cohort study of 724 consecutive patients
- PMID: 24244441
- PMCID: PMC3828295
- DOI: 10.1371/journal.pone.0079170
Reduction of thromboembolic events in meningioma surgery: a cohort study of 724 consecutive patients
Abstract
Background: Meningiomas are associated with the highest postoperative rate of venous thromboembolic events (VTE) among all intracranial tumors. The aim of this study is to compare two entirely different VTE prophylaxis regimens in 724 consecutive patients undergoing meningioma surgery.
Methods: Two cohorts at a single institution treated with different regimens to prevent VTE were reviewed retrospectively. Cohort A (n = 482; 314 females, mean age 57 years, range: 11-87 years) received our institutional regimen during the years 1999-2006, consisting of low-molecular-weight heparin (LMWH) and compression stockings. For cohort B (n = 242; 163 females, mean age 56.8 years, range: 16-90 years), during the years 2008-2010, the management included intraoperative 10°-20° leg elevation with intermittent pneumatic compression (IPC), heparin and LMWH administration. We compared the incidence of the endpoints pulmonary embolism (PE), deep venous thrombosis (DVT), hemorrhage and death, taking into account several known associated risk factors.
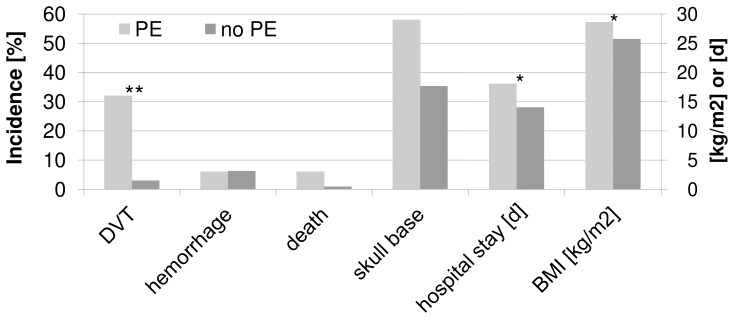
Results: For all endpoints, we observed a more favorable outcome with the new regimen. The difference in incidence of PEs (cohort A: 38/482, 8%; cohort B: 6/242, 2.5%) reached statistical significance (p = 0.002). In general, patients with skull base meningiomas had a higher risk for PE (OR 2.77). Regarding VTE prophylaxis, an adjusted subgroup analysis suggests that the new regimen is particularly beneficial for patients with skull base meningiomas.
Conclusions: We recommend perioperative prophylaxis using a management composed of intraoperative leg-elevation, IPC, early heparin administration and LMWH to reduce the risk for PE.
Conflict of interest statement
Figures




References
-
- Gerber DE, Segal JB, Salhotra A, Olivi A, Grossman SA, et al. (2007) Venous thromboembolism occurs infrequently in meningioma patients receiving combined modality prophylaxis. Cancer 109: 300–305. - PubMed
-
- Caroli M, Locatelli M, Prada F, Beretta F, Martinelli-Boneschi F, et al. (2005) Surgery for intracranial meningiomas in the elderly: a clinical-radiological grading system as a predictor of outcome. J Neurosurg 102: 290–294. - PubMed
-
- Sawaya R, Decourteen-Meyers G, Copeland B (1984) Massive preoperative pulmonary embolism and suprasellar brain tumor: case report and review of the literature. Neurosurgery 15: 566–571. - PubMed
-
- Al-Mefty O (1991) MENINGIOMAS. XXI+630P p.
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
