

Stenting and medical therapy for atherosclerotic renal-artery stenosis
- PMID: 24245566
- PMCID: PMC4815927
- DOI: 10.1056/NEJMoa1310753
Stenting and medical therapy for atherosclerotic renal-artery stenosis
Abstract
Background: Atherosclerotic renal-artery stenosis is a common problem in the elderly. Despite two randomized trials that did not show a benefit of renal-artery stenting with respect to kidney function, the usefulness of stenting for the prevention of major adverse renal and cardiovascular events is uncertain.
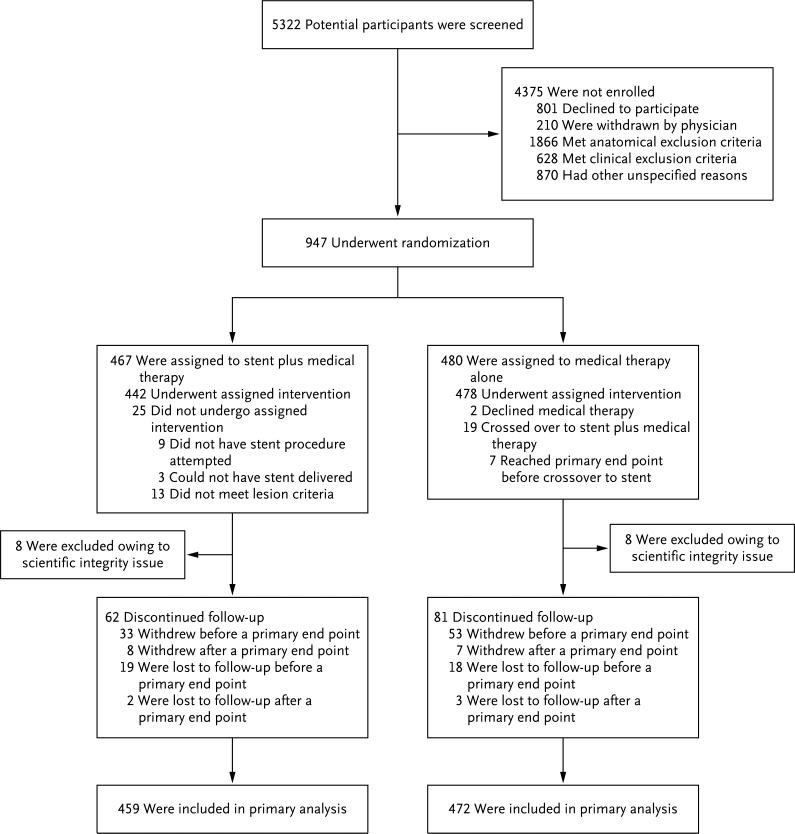
Methods: We randomly assigned 947 participants who had atherosclerotic renal-artery stenosis and either systolic hypertension while taking two or more antihypertensive drugs or chronic kidney disease to medical therapy plus renal-artery stenting or medical therapy alone. Participants were followed for the occurrence of adverse cardiovascular and renal events (a composite end point of death from cardiovascular or renal causes, myocardial infarction, stroke, hospitalization for congestive heart failure, progressive renal insufficiency, or the need for renal-replacement therapy).
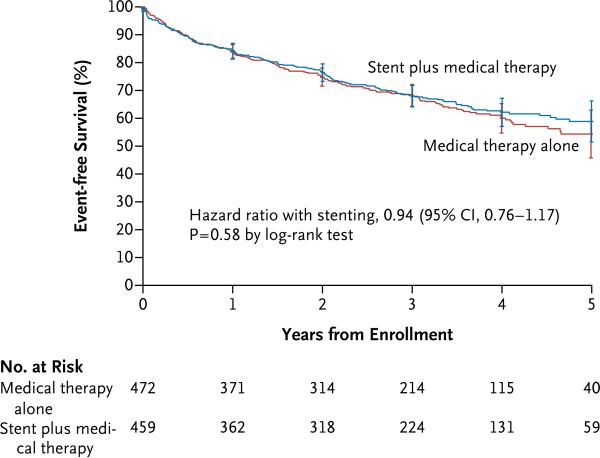
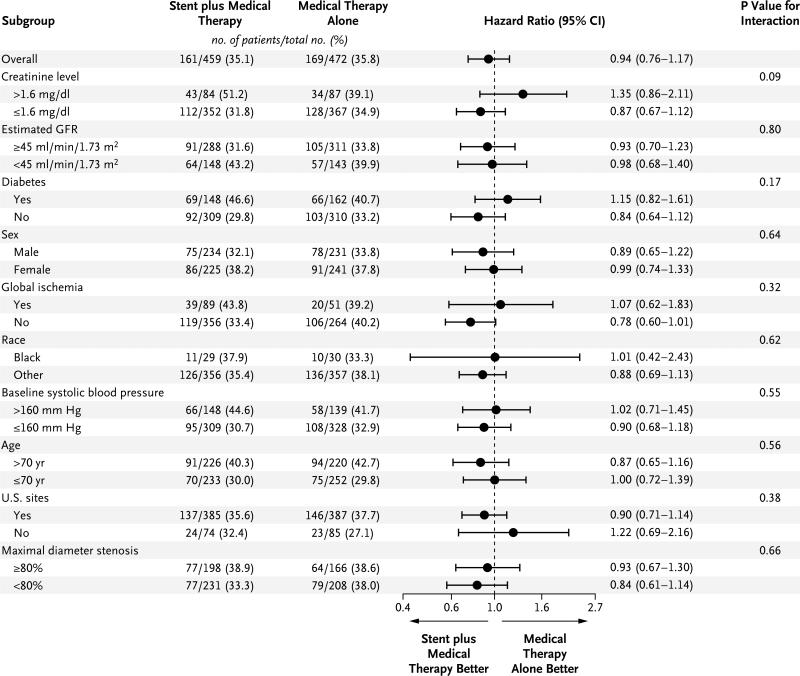
Results: Over a median follow-up period of 43 months (interquartile range, 31 to 55), the rate of the primary composite end point did not differ significantly between participants who underwent stenting in addition to receiving medical therapy and those who received medical therapy alone (35.1% and 35.8%, respectively; hazard ratio with stenting, 0.94; 95% confidence interval [CI], 0.76 to 1.17; P=0.58). There were also no significant differences between the treatment groups in the rates of the individual components of the primary end point or in all-cause mortality. During follow-up, there was a consistent modest difference in systolic blood pressure favoring the stent group (-2.3 mm Hg; 95% CI, -4.4 to -0.2; P=0.03).
Conclusions: Renal-artery stenting did not confer a significant benefit with respect to the prevention of clinical events when added to comprehensive, multifactorial medical therapy in people with atherosclerotic renal-artery stenosis and hypertension or chronic kidney disease. (Funded by the National Heart, Lung and Blood Institute and others; ClinicalTrials.gov number, NCT00081731.).
Figures
Comment in
-
Treatment of atherosclerotic renovascular disease.N Engl J Med. 2014 Jan 2;370(1):78-9. doi: 10.1056/NEJMe1313423. Epub 2013 Nov 18. N Engl J Med. 2014. PMID: 24245567 No abstract available.
-
Is time of renal hypoperfusion an important variable in determining response to renal artery revascularization?JACC Cardiovasc Interv. 2014 Jan;7(1):110. doi: 10.1016/j.jcin.2013.12.001. JACC Cardiovasc Interv. 2014. PMID: 24456726 No abstract available.
-
Do kidneys need blood?Eur J Vasc Endovasc Surg. 2014 May;47(5):459-60. doi: 10.1016/j.ejvs.2013.12.019. Epub 2014 Feb 11. Eur J Vasc Endovasc Surg. 2014. PMID: 24524813 No abstract available.
-
Stenting for renal-artery stenosis.N Engl J Med. 2014 May 8;370(19):1854-5. doi: 10.1056/NEJMc1402687. N Engl J Med. 2014. PMID: 24806166 Free PMC article. No abstract available.
-
Stenting for renal-artery stenosis.N Engl J Med. 2014 May 8;370(19):1852. doi: 10.1056/NEJMc1402687. N Engl J Med. 2014. PMID: 24806167 No abstract available.
-
Stenting for renal-artery stenosis.N Engl J Med. 2014 May 8;370(19):1852-3. doi: 10.1056/NEJMc1402687. N Engl J Med. 2014. PMID: 24806168 No abstract available.
-
Stenting for renal-artery stenosis.N Engl J Med. 2014 May 8;370(19):1853. doi: 10.1056/NEJMc1402687. N Engl J Med. 2014. PMID: 24806169 No abstract available.
-
Stenting for renal-artery stenosis.N Engl J Med. 2014 May 8;370(19):1853-4. doi: 10.1056/NEJMc1402687. N Engl J Med. 2014. PMID: 24806170 No abstract available.
-
Stenting for renal-artery stenosis.N Engl J Med. 2014 May 8;370(19):1854. doi: 10.1056/NEJMc1402687. N Engl J Med. 2014. PMID: 24806171 No abstract available.
-
What is the optimal treatment for patients with atherosclerotic renal artery stenosis?Am J Kidney Dis. 2014 Aug;64(2):174-7. doi: 10.1053/j.ajkd.2014.04.003. Epub 2014 May 10. Am J Kidney Dis. 2014. PMID: 24815771 No abstract available.
References
-
- Derkx FH, Schalekamp MA. Renal artery stenosis and hypertension. Lancet. 1994;344:237–9. - PubMed
-
- Ram CV. Renovascular hypertension. Curr Opin Nephrol Hypertens. 1997;6:575–9. - PubMed
-
- Olin JW, Melia M, Young JR, Graor RA, Risius B. Prevalence of atherosclerotic renal artery stenosis in patients with atherosclerosis elsewhere. Am J Med. 1990;88:46N–51N. - PubMed
-
- Harding MB, Smith LR, Himmelstein SI, et al. Renal artery stenosis: prevalence and associated risk factors in patients undergoing routine cardiac catheterization. J Am Soc Nephrol. 1992;2:1608–16. - PubMed
-
- Hansen KJ, Edwards MS, Craven TE, et al. Prevalence of renovascular disease in the elderly: a population-based study. J Vasc Surg. 2002;36:443–51. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical