

Numbers matter to informed patient choices: a randomized design across age and numeracy levels
- PMID: 24246563
- PMCID: PMC3991753
- DOI: 10.1177/0272989X13511705
Numbers matter to informed patient choices: a randomized design across age and numeracy levels
Abstract
Background: How drug adverse events (AEs) are communicated in the United States may mislead consumers and result in low adherence. Requiring written information to include numeric AE-likelihood information might lessen these effects, but providing numbers may disadvantage less skilled populations. The objective was to determine risk comprehension and willingness to use a medication when presented with numeric or nonnumeric AE-likelihood information across age, numeracy, and cholesterol-lowering drug-use groups.
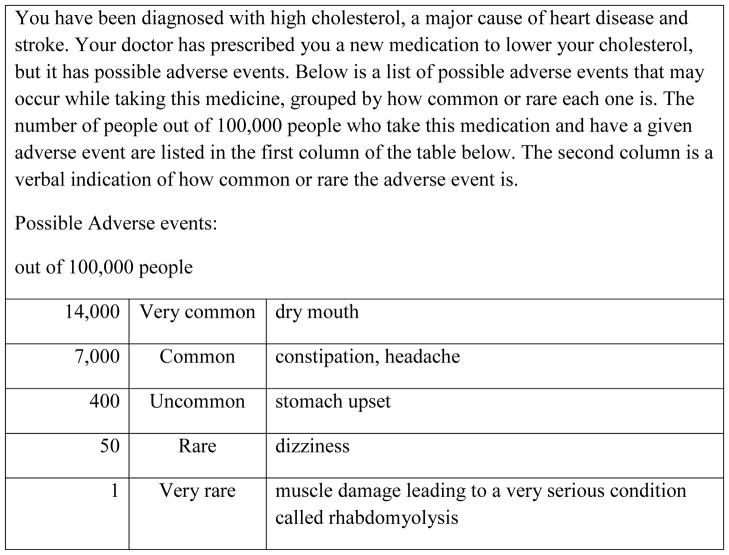
Methods: In a cross-sectional Internet survey (N = 905; American Life Panel, 15 May 2008 to 18 June 2008), respondents were presented with a hypothetical prescription medication for high cholesterol. AE likelihoods were described using 1 of 6 formats (nonnumeric: consumer medication information (CMI)-like list, risk labels; numeric: percentage, frequency, risk labels + percentage, risk labels + frequency). Main outcome measures were risk comprehension (recoded to indicate presence/absence of risk overestimation and underestimation), willingness to use the medication (7-point scale; not likely = 0, very likely = 6), and main reason for willingness (chosen from 8 predefined reasons).
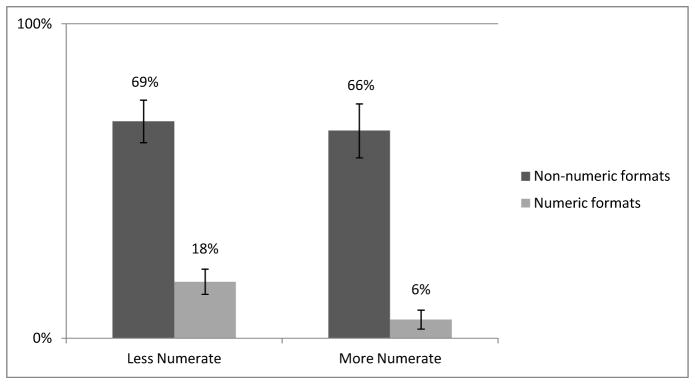
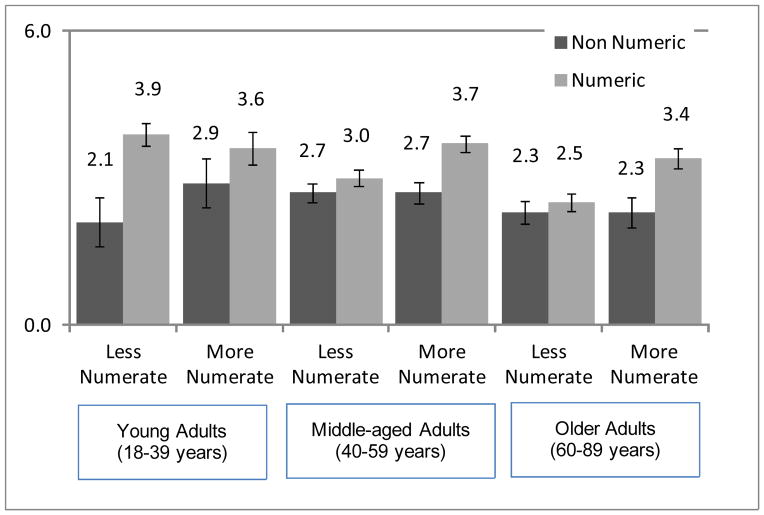
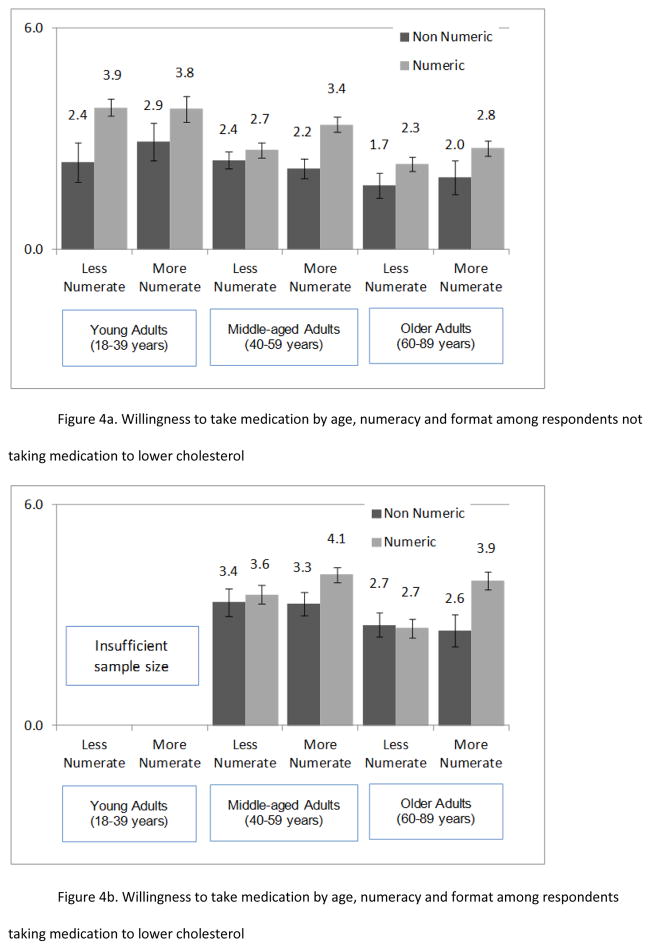
Results: Individuals given nonnumeric information were more likely to overestimate risk, were less willing to take the medication, and gave different reasons than those provided numeric information across numeracy and age groups (e.g., among the less numerate, 69% and 18% overestimated risks in nonnumeric and numeric formats, respectively; among the more numerate, these same proportions were 66% and 6%). Less numerate middle-aged and older adults, however, showed less influence of numeric format on willingness to take the medication. It is unclear whether differences are clinically meaningful, although some differences are large.
Conclusions: Providing numeric AE-likelihood information (compared with nonnumeric) is likely to increase risk comprehension across numeracy and age levels. Its effects on uptake and adherence of prescribed drugs should be similar across the population, except perhaps in older, less numerate individuals.
Keywords: adherence; aging; informed decision making; numeracy; pharmaceutical decision making; risk communication; risk comprehension; statins.
Figures
References
-
- World Health Organization. [Accessed August 22, 2012.];Adherence to long-term therapies: evidence for action. http://www.who.int/chp/knowledge/publications/adherence_report/en/. Published 2003.
-
- Katz JN, Daltroy LH, Brennan TA, Liang MH. Informed consent and the prescription of nonsteroidal antiinflammatory drugs. Arthritis Rheum. 1992;35(11):1257–1263. - PubMed
-
- Sleath B, Tulsky JA, Peck BM, Thorpe J. Provider-patient communication about antidepressants among veterans with mental health conditions. Am J Geriatr Pharmacother. 2007;5(1):9–17. - PubMed
-
- Tarn DM, Heritage J, Paterniti DA, Hays RD, Kravitz RL, Wenger NS. Physician communication when prescribing new medications. Arch Intern Med. 2006;166(17):1855–1862. - PubMed
-
- Ziegler DK, Mosier MC, Buenaver M, Okuyemi K. How much information about adverse effects of medication do patients want from physicians? Arch Intern Med. 2001;161(5):706–713. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
