

Staphylococcus aureus bloodstream infection: a pooled analysis of five prospective, observational studies
- PMID: 24247070
- PMCID: PMC4136490
- DOI: 10.1016/j.jinf.2013.10.015
Staphylococcus aureus bloodstream infection: a pooled analysis of five prospective, observational studies
Erratum in
- J Infect. 2014 Sep;69(3):306-7
Abstract
Objectives: Staphylococcus aureus bacteraemia is a common, often fatal infection. Our aim was to describe how its clinical presentation varies between populations and to identify common determinants of outcome.
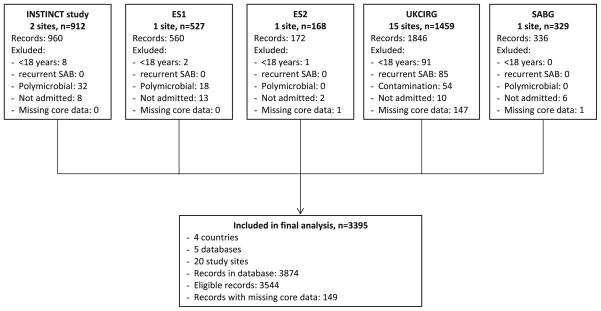
Methods: We conducted a pooled analysis on 3395 consecutive adult patients with S. aureus bacteraemia. Patients were enrolled between 2006 and 2011 in five prospective studies in 20 tertiary care centres in Germany, Spain, United Kingdom, and United States.
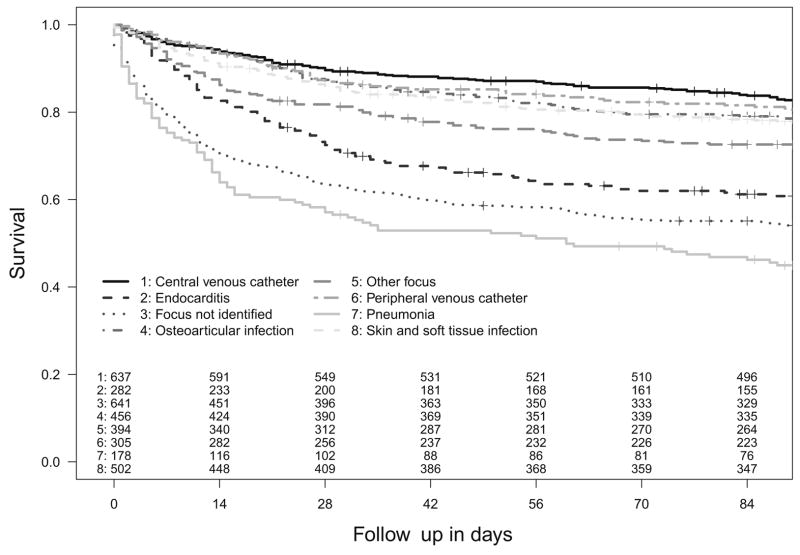
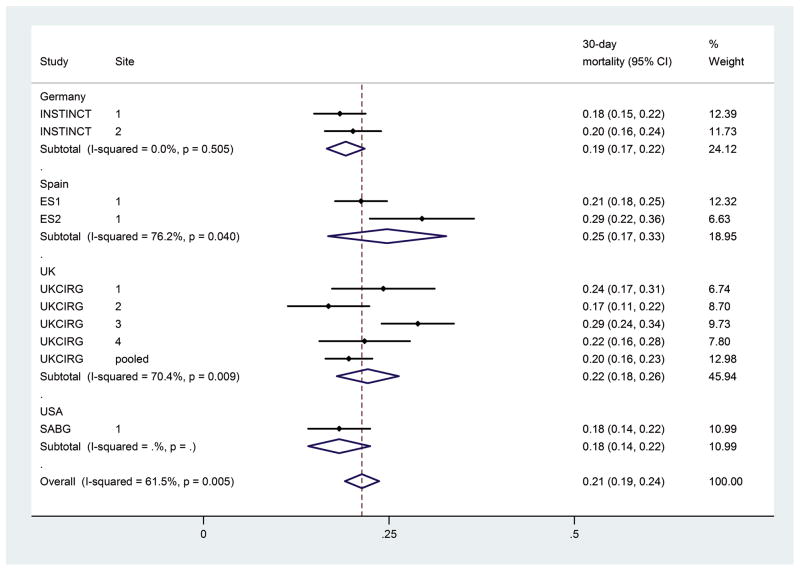
Results: The median age of participants was 64 years (interquartile range 50-75 years) and 63.8% were male. 25.4% of infections were associated with diabetes mellitus, 40.7% were nosocomial, 20.6% were caused by methicillin-resistant S. aureus (MRSA), although these proportions varied significantly across studies. Intravenous catheters were the commonest identified infective focus (27.7%); 8.3% had endocarditis. Crude 14 and 90-day mortality was 14.6% and 29.2%, respectively. Age, MRSA bacteraemia, nosocomial acquisition, endocarditis, and pneumonia were independently associated with death, but a strong association was with an unidentified infective focus (adjusted hazard ratio for 90-day mortality 2.92; 95% confidence interval 2.33 to 3.67, p < 0.0001).
Conclusion: The baseline demographic and clinical features of S. aureus bacteraemia vary significantly between populations. Mortality could be reduced by assiduous MRSA control and early identification of the infective focus.
Keywords: Bacteraemia; Mortality; Pooled analysis; Staphylococcus aureus bloodstream infection.
Copyright © 2013 The British Infection Association. Published by Elsevier Ltd. All rights reserved.
Conflict of interest statement
J.E. and H.S. serve on an advisory committee for Basilea Pharmaceutica International, V.G.F. for Merck, A.P.R.W. for Quintiles and Momentum, H.S. for Astellas, Astra Zeneca, Cubist, 3M Medica, Novartis, and Theravance. V.G.F. was a paid consultant for Pfizer, Novartis, Galderma, Novadigm, Durata, Achaogen, Affinium, Medicines Co., Cerexa, and MedImmune, H.S. for Astellas, Basilea, Gilead, MSD Sharp & Dohme, Pfizer, and SIRS-Lab, J.R.B. for Roche, Merck, Janssen-Cilag, Pfizer, and Novartis. V.G.F. has received research grants or support from Merck, Theravance, Cerexa, Pfizer, Medimmune, Novartis, NIH, and Advanced Liquid Logics, J.R.B. from Novartis, H.S. from Basilea, and Novartis. J.R.B. has received payments for lectures from Merck, Astellas, Pfizer, AstraZeneca, and Novartis; H.S. from Astellas, Astra Zeneca, Gilead, MSD Sharp&Dohme, Novartis, Pfizer, and Oxoid, A.J.K. from BD Biosciences, Biomérieux, MSD Sharp & Dohme, and ViiV Healthcare, A.S. from Novartis and Pfizer. V.G.F. holds a patent on NCGR. V.G.F. has received royalties from UpToDate, M.E.T. from Oxford University Press. V.G.F. has been paid for developing and delivering educational presentations for Cubist, Cerexa, and Theravance. S.R. has received travel support from Astellas and MSD Sharp & Dohme, A.J.K. from Janssen-Cila, and. M.E.T from Illumina Inc. All other authors: no other relationships or activities that could appear to have influenced the submitted work.
Figures
References
-
- Laupland KB. Incidence of bloodstream infection: a review of population-based studies. Clin Microbiol Infect. 2013;19(6):492–500. - PubMed
-
- Thwaites GE, Edgeworth JD, Gkrania-Klotsas E, Kirby A, Tilley R, Torok ME, et al. Clinical management of Staphylococcus aureus bacteraemia. Lancet Infect Dis. 2011;11(3):208–22. - PubMed
-
- Kern WV. Management of Staphylococcus aureus bacteremia and endocarditis: progresses and challenges. Curr Opin Infect Dis. 2010;23(4):346–58. - PubMed
-
- Rieg S, Peyerl-Hoffmann G, de With K, Theilacker C, Wagner D, Hubner J, et al. Mortality of S. aureus bacteremia and infectious diseases specialist consultation – a study of 521 patients in Germany. J Infect. 2009;59(4):232–9. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
