

Low-dose dopamine or low-dose nesiritide in acute heart failure with renal dysfunction: the ROSE acute heart failure randomized trial
- PMID: 24247300
- PMCID: PMC3934929
- DOI: 10.1001/jama.2013.282190
Low-dose dopamine or low-dose nesiritide in acute heart failure with renal dysfunction: the ROSE acute heart failure randomized trial
Abstract
Importance: Small studies suggest that low-dose dopamine or low-dose nesiritide may enhance decongestion and preserve renal function in patients with acute heart failure and renal dysfunction; however, neither strategy has been rigorously tested.
Objective: To test the 2 independent hypotheses that, compared with placebo, addition of low-dose dopamine (2 μg/kg/min) or low-dose nesiritide (0.005 μg/kg/min without bolus) to diuretic therapy will enhance decongestion and preserve renal function in patients with acute heart failure and renal dysfunction.
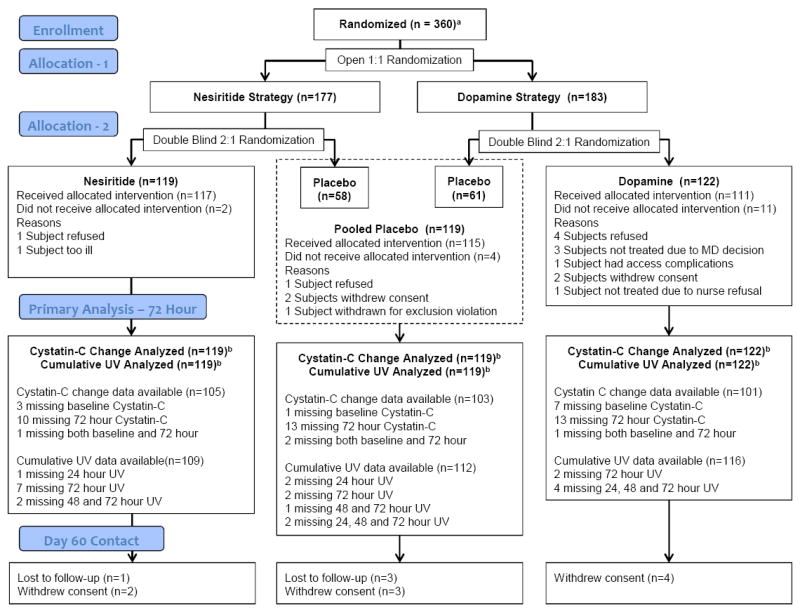
Design, setting, and participants: Multicenter, double-blind, placebo-controlled clinical trial (Renal Optimization Strategies Evaluation [ROSE]) of 360 hospitalized patients with acute heart failure and renal dysfunction (estimated glomerular filtration rate of 15-60 mL/min/1.73 m2), randomized within 24 hours of admission. Enrollment occurred from September 2010 to March 2013 across 26 sites in North America.
Interventions: Participants were randomized in an open, 1:1 allocation ratio to the dopamine or nesiritide strategy. Within each strategy, participants were randomized in a double-blind, 2:1 ratio to active treatment or placebo. The dopamine (n = 122) and nesiritide (n = 119) groups were independently compared with the pooled placebo group (n = 119).
Main outcomes and measures: Coprimary end points included 72-hour cumulative urine volume (decongestion end point) and the change in serum cystatin C from enrollment to 72 hours (renal function end point).
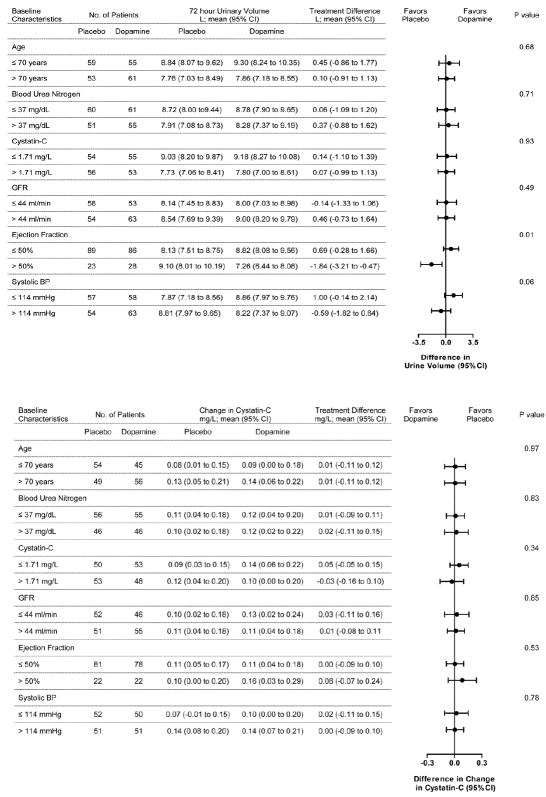
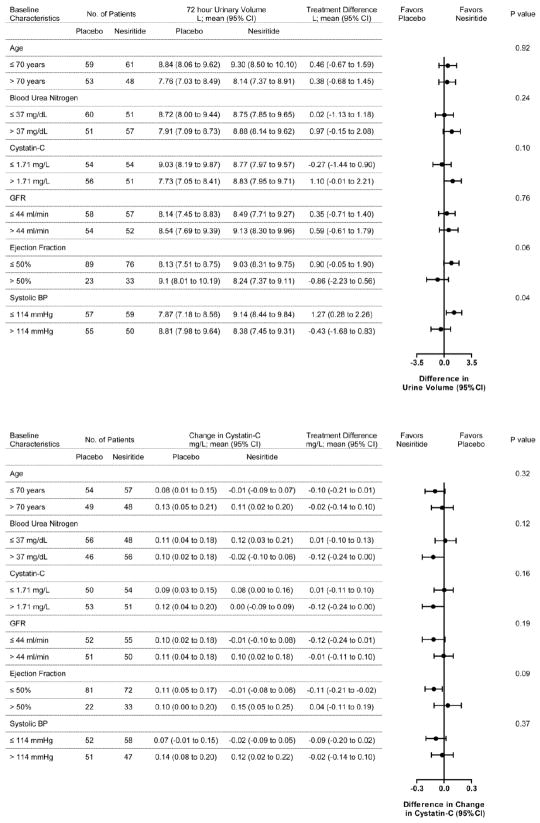
Results: Compared with placebo, low-dose dopamine had no significant effect on 72-hour cumulative urine volume (dopamine, 8524 mL; 95% CI, 7917-9131 vs placebo, 8296 mL; 95% CI, 7762-8830 ; difference, 229 mL; 95% CI, -714 to 1171 mL; P = .59) or on the change in cystatin C level (dopamine, 0.12 mg/L; 95% CI, 0.06-0.18 vs placebo, 0.11 mg/L; 95% CI, 0.06-0.16; difference, 0.01; 95% CI, -0.08 to 0.10; P = .72). Similarly, low-dose nesiritide had no significant effect on 72-hour cumulative urine volume (nesiritide, 8574 mL; 95% CI, 8014-9134 vs placebo, 8296 mL; 95% CI, 7762-8830; difference, 279 mL; 95% CI, -618 to 1176 mL; P = .49) or on the change in cystatin C level (nesiritide, 0.07 mg/L; 95% CI, 0.01-0.13 vs placebo, 0.11 mg/L; 95% CI, 0.06-0.16; difference, -0.04; 95% CI, -0.13 to 0.05; P = .36). Compared with placebo, there was no effect of low-dose dopamine or nesiritide on secondary end points reflective of decongestion, renal function, or clinical outcomes.
Conclusion and relevance: In participants with acute heart failure and renal dysfunction, neither low-dose dopamine nor low-dose nesiritide enhanced decongestion or improved renal function when added to diuretic therapy.
Trial registration: clinicaltrials.gov Identifier: NCT01132846.
Conflict of interest statement
HH Chen: Dr. Chen
KJ Anstrom: Dr. Anstrom
MM Givertz: Dr. Givertz
LW Stevenson: Dr. Stevenson
MJ Semigran: Dr. Semigran
SR Goldsmith: Dr. Goldsmith
BA Bart: Dr. Bart
DA Bull: Dr. Bull
J Stehlik: Dr. Stehlik
MM LeWinter: Dr. LeWinter
MA Konstam: Dr. Konstam
GS Huggins: Dr. Huggins
JL Rouleau: Dr. Rouleau
E O’Meara: Dr. O’Meara
WHW Tang: Dr. Tang
RC Starling: Dr. Starling
J Butler: Dr. Butler
A Deswal: Dr. Deswal
GM Felker: Dr. Felker
CM O’Connor: Dr. O’Connor
RE Bonita: Dr. Bonita
KB Margulies: Dr. Margulies
TP Cappola: Dr. Cappola
EO Ofili: Dr. Ofili
DL Mann: Dr. Mann
VG Davila-Roman: Dr. Davila-Roman
SE McNulty: Dr. McNulty
BA Borlaug: Dr. Borlaug
EJ Velazquez: Dr. Velazquez
KL Lee: Dr. Lee
MR Shah: Dr. Shah
AF Hernandez: Dr. Hernandez
E Braunwald: Dr. Braunwald
MM Redfield: Dr. Redfield
Figures
Comment in
-
Heart failure: addition of vasodilators to diuretic therapy does not improve outcome in acute heart failure.Nat Rev Cardiol. 2014 Jan;11(1):4. doi: 10.1038/nrcardio.2013.189. Epub 2013 Dec 3. Nat Rev Cardiol. 2014. PMID: 24302220 No abstract available.
-
[The ROSE study].G Ital Cardiol (Rome). 2014 Jan;15(1):9-12. doi: 10.1714/1394.15512. G Ital Cardiol (Rome). 2014. PMID: 24503728 Italian. No abstract available.
-
Calling for targeted trials in cardiorenal syndromes.Am J Kidney Dis. 2014 Jul;64(1):10-2. doi: 10.1053/j.ajkd.2014.03.006. Epub 2014 Apr 6. Am J Kidney Dis. 2014. PMID: 24713221 No abstract available.
-
Dopamine vs nesiritide for acute heart failure with renal dysfunction.JAMA. 2014 Apr 16;311(15):1565. doi: 10.1001/jama.2014.2459. JAMA. 2014. PMID: 24737371 No abstract available.
-
Dopamine vs nesiritide for acute heart failure with renal dysfunction--reply.JAMA. 2014 Apr 16;311(15):1565-6. doi: 10.1001/jama.2014.2462. JAMA. 2014. PMID: 24737372 No abstract available.
References
-
- Lindenfeld J, Albert NM, Boehmer JP, et al. HFSA 2010 Comprehensive Heart Failure Practice Guideline. J Card Fail. 2010;16(6):e1–194. - PubMed
-
- Yancy CW, Jessup M, Bozkurt B, et al. 2013 ACCF/AHA Guideline for the Management of Heart Failure: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation. 2013 doi: 10.1161/CIR.0b013e31829e8776 3. - PubMed
-
- Givertz MM, Teerlink JR, Albert NM, et al. Acute decompensated heart failure: update on new and emerging evidence and directions for future research. J Card Fail. 2013;19(6):371–389. - PubMed
-
- Maskin CS, Ocken S, Chadwick B, LeJemtel TH. Comparative systemic and renal effects of dopamine and angiotensin-converting enzyme inhibition with enalaprilat in patients with heart failure. Circulation. 1985;72(4):846–852. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
- U01 HL084890/HL/NHLBI NIH HHS/United States
- U01 HL084891/HL/NHLBI NIH HHS/United States
- U01 HL084931/HL/NHLBI NIH HHS/United States
- U10 HL110342/HL/NHLBI NIH HHS/United States
- U0-1 HL084861/HL/NHLBI NIH HHS/United States
- UL1 TR000454/TR/NCATS NIH HHS/United States
- Z99 HL999999/ImNIH/Intramural NIH HHS/United States
- UL1TR000439/TR/NCATS NIH HHS/United States
- U10 HL110337/HL/NHLBI NIH HHS/United States
- 8 U54 MD007588/MD/NIMHD NIH HHS/United States
- R01 HL084155/HL/NHLBI NIH HHS/United States
- U10 HL110336/HL/NHLBI NIH HHS/United States
- U10 HL110338/HL/NHLBI NIH HHS/United States
- UL1TR000135/TR/NCATS NIH HHS/United States
- U54 MD007588/MD/NIMHD NIH HHS/United States
- UL1TR000454/TR/NCATS NIH HHS/United States
- U01 HL084861/HL/NHLBI NIH HHS/United States
- U10 HL084904/HL/NHLBI NIH HHS/United States
- U10 HL110312/HL/NHLBI NIH HHS/United States
- UL1RR025008/RR/NCRR NIH HHS/United States
- UL1 TR000135/TR/NCATS NIH HHS/United States
- K23 HL095661/HL/NHLBI NIH HHS/United States
- UL1 TR000439/TR/NCATS NIH HHS/United States
- U10 HL110262/HL/NHLBI NIH HHS/United States
- U109 HL110337/HL/NHLBI NIH HHS/United States
- UL1 RR025008/RR/NCRR NIH HHS/United States
- U10 HL110302/HL/NHLBI NIH HHS/United States
- U10 HL110297/HL/NHLBI NIH HHS/United States
- U01 HL084889/HL/NHLBI NIH HHS/United States
- U10 HL110309/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
