

Physical complications in acute lung injury survivors: a two-year longitudinal prospective study
- PMID: 24247473
- PMCID: PMC3959239
- DOI: 10.1097/CCM.0000000000000040
Physical complications in acute lung injury survivors: a two-year longitudinal prospective study
Abstract
Objective: Survivors of severe critical illness frequently develop substantial and persistent physical complications, including muscle weakness, impaired physical function, and decreased health-related quality of life. Our objective was to determine the longitudinal epidemiology of muscle weakness, physical function, and health-related quality of life and their associations with critical illness and ICU exposures.
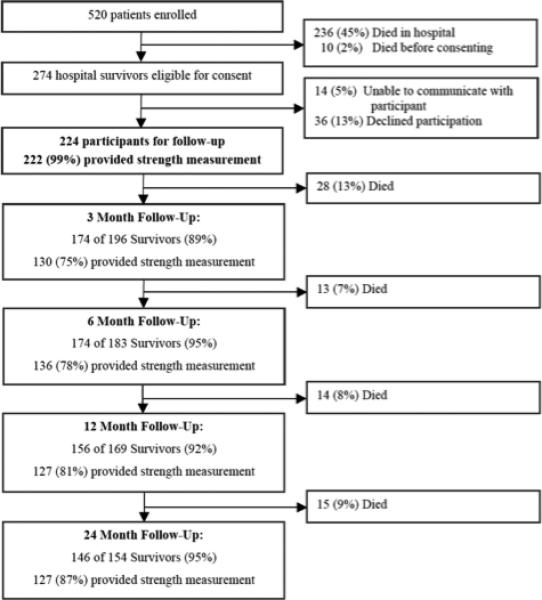
Design: A multisite prospective study with longitudinal follow-up at 3, 6, 12, and 24 months after acute lung injury.
Setting: Thirteen ICUs from four academic teaching hospitals.
Patients: Two hundred twenty-two survivors of acute lung injury.
Interventions: None.
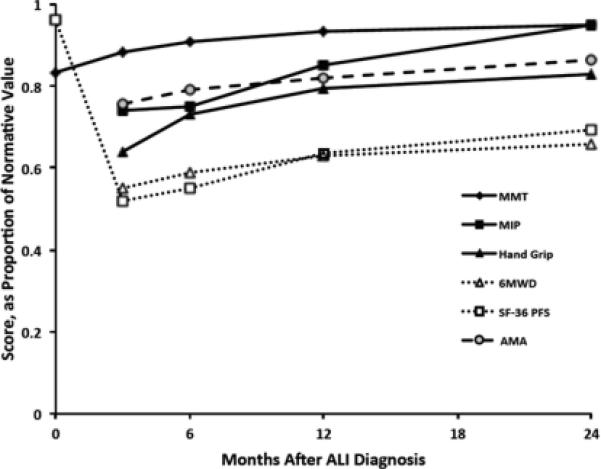
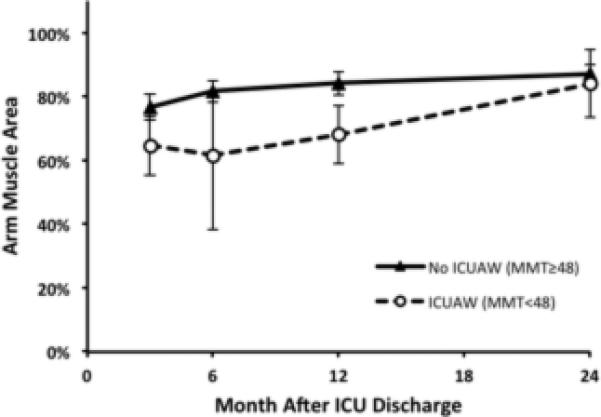
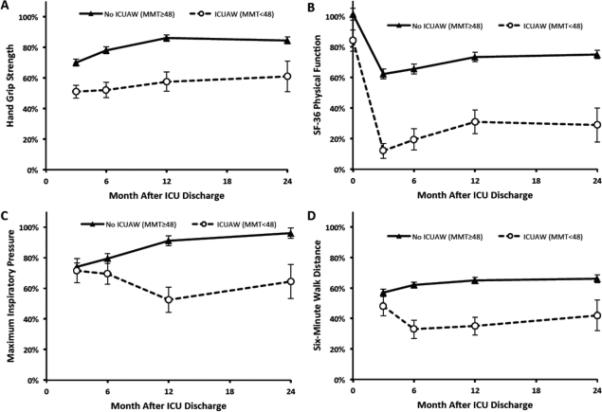
Measurements and main results: At each time point, patients underwent standardized clinical evaluations of extremity, hand grip, and respiratory muscle strength; anthropometrics (height, weight, mid-arm circumference, and triceps skin fold thickness); 6-minute walk distance, and the Medical Outcomes Short-Form 36 health-related quality of life survey. During their hospitalization, survivors also had detailed daily evaluation of critical illness and related treatment variables. Over one third of survivors had objective evidence of muscle weakness at hospital discharge, with most improving within 12 months. This weakness was associated with substantial impairments in physical function and health-related quality of life that persisted at 24 months. The duration of bed rest during critical illness was consistently associated with weakness throughout 24-month follow-up. The cumulative dose of systematic corticosteroids and use of neuromuscular blockers in the ICU were not associated with weakness.
Conclusions: Muscle weakness is common after acute lung injury, usually recovering within 12 months. This weakness is associated with substantial impairments in physical function and health-related quality of life that continue beyond 24 months. These results provide valuable prognostic information regarding physical recovery after acute lung injury. Evidence-based methods to reduce the duration of bed rest during critical illness may be important for improving these long-term impairments.
Figures
References
-
- Martin GS, Mannino DM, Eaton S, et al. The epidemiology of sepsis in the United States from 1979 through 2000. N Engl J Med 2003. 348:1546–1554. - PubMed
-
- Zambon M, Vincent J-L. Mortality rates for patients with acute lung injury/ARDS have decreased over time. Chest. 2008;133:1120–1127. - PubMed
-
- Carson SS, Cox CE, Holmes GM, et al. The changing epidemiology of mechanical ventilation: a population-based study. Journal of Intensive Care Medicine. 2006;21:173–182. - PubMed
-
- Needham DM, Bronskill SE, Rothwell DM, et al. Hospital volume and mortality for mechanical ventilation of medical and surgical patients: a population-based analysis using administrative data. Crit Care Med. 2006;34:2349–2354. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
